Vol 1 | Issue 1 | July – Sep 2015 | page:4-5 | Shiv Kumar Singh [1].
Author: Dr. Shiv Kumar Singh [1].
[1]Royal Liverpool University Hospitals Prescot Street Liverpool L7 8XP.
Address of Correspondence
Dr. Shiv Kumar Singh.
Royal Liverpool University Hospitals,
Prescot Street,
Liverpool L7 8XP.
Email: shvkmrsngh@aol.com
Editorial: Safety in Anaesthesia
Management of acute pain is important part of peri-op care and use of nerve blocks not only provide good peri-op pain relief but they also help in reducing the requirements for opioids and their associated complication like sedation and PONV (Post-Op Nausea and Vomiting). There are places in this world where, leave alone US machines, even Peripheral Nerve Stimulators (PNS) are not available to the practicing anaesthetist. Blind blocks using paraesthesia are still practiced for some of the plexus blocks. There are certain other blocks that can be done in patients with just feel of a blunt needle passing through fascial layers, namely Intermediate cervical plexus block, Paravertebral Blocks, Transversus Abdominis Plane Blocks, Rectus Sheath Blocks, Ilioinguinal Nerve Blocks and Fascia Iliaca Block. These are called Loss of Resistance (LOR) Blocks.
The efficacy of any of these blocks depends on depositing LA in the right plane. There are many factors that can lead to deposition of LA in the wrong plane and increased incidence of failure and complications. Foremost, it is important to have a good knowledge of the anatomy of the region where the blocks are to be done. It is equally important to have knowledge of the surgical anatomy; the good block you have given, will not work if it does not cover the surgical field that includes dermatomes, myotomes and osteotomes (for orthopaedic procedures). For abdominal procedures, it is important to remember that the pain arises from both somatic and visceral components. The LA blocks cover the pain arising from the somatic, but not the visceral component. For the visceral pain it is necessary to use combination of simple analgesics and opioids. Where these rules are not followed, failures occur.
As far as the blocks are concerned, understanding “Cushion Effect” is the most important concept that needs to be understood. The “Cushion Effect” occurs due to the use of “blunt” needles. We first described this effect in a paper published in Anaesthesia in 2007. [1] The needles used for the LOR are blunt or short beveled and therefore a considerable amount of force is required for the tip of the needle to pierce the skin. This large amount of force tends to obliterate the cushion of subcutaneous fat lying under the skin, the “cushion effect”, and as the skin barrier is breached, the needle passes not only through the skin but also through the subcutaneous tissues and the fascia. [Fig-1] This may lead to feeling “pops” in a wrong/deeper planes and deposition of local anaesthetic in the wrong place with failure and some time complications (like femoral nerve block while performing hernia blocks), something which is not expected.
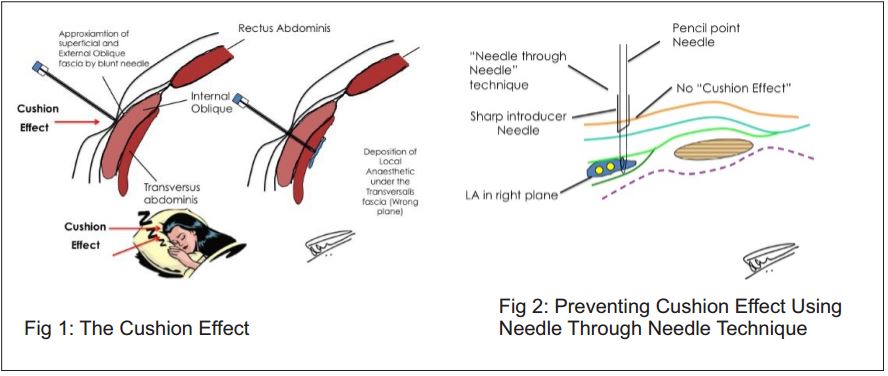
There are mainly three ways in which the “Cushion Effect” can be prevented. In the first method, before introducing the LOR needle,a small nick in the skin is made through the skin with a sharper bigger needle or a surgical blade. In the second method, described by us in the article published in Anaesthesia, we use “needle through needle” technique. In this technique the LOR needle is passed through a larger sharp needle (the introducer). [Fig-2] In the last method, we assume that the needle has overshot due to the “cushion effect” and all we do is, once the needle has pierced the skin, we withdraw the needle back till the tip of the needle is just under it and then start feeling the loss of resistance. In all cases, before feeling the loss of resistance, it is always nice to feel the “bounce” on the fascia before feeling the “pop.The details of various LOR techniques can be read in our article (free access), the loss of resistance blocks. [2]
In conclusion, understanding the anatomy and avoiding the “cushion effect” helps to perform the loss of resistance blocks with greater confidence and excellent results. Simplicity of these blocks allows them to be performed in the theatres but also be used as “rescue analgesics” in situations where pain can be difficult to control in the post-op period. Loss of resistance techniques are not only easy to learn (and teach) but due to minimal resources required, they are highly cost effective too.
Shiv Kumar Singh
References
1. Craig RG and Singh SK. A new technique for ilioinguinal and iliohypogastric nerve block. Anaesthesia 2007; 96-97.
2. Singh SK and Gulyam Kuruba SM. The loss of resistance nerve blocks. ISRN Anesthesiology 2011; Article ID 421505.
| How to Cite this Article: Singh S K. Just A Needle and Some Local Anaesthetic to Relieve Acute Pain, The Loss of Resistance Blocks. Journal of Anaesthesia and Critical Care Case Reports July-Sep 2015; 1(1):4-5. |
(Abstract) (Full Text HTML) (Download PDF)