Case Report | Vol 11 | Issue 2 | May-August 2025 | Page: 04-06 | Jayal Bhagat, Himani Patel, Piyush Desai
DOI: https://doi.org/10.13107/jaccr.2025.v11.i02.272
Open Access License: CC BY-NC 4.0
Copyright Statement: Copyright © 2025; The Author(s).
Submitted: 29/04/2025; Reviewed: 15/05/2025; Accepted: 22/07/2025; Published: 10/08/2025
Author: Jayal Bhagat [1], Himani Patel [1], Piyush Desai [1]
[1] Department of Anaesthesia, UNM Children Hospital, Surat, Gujarat, India.
Address of Correspondence
Dr. Himani Patel,
Paediatric Anaesthetist, UNM Children Hospital, Surat, Gujarat, India.
E-mail: phimani494@yahoo.com
Abstract
This case report describes the successful anaesthetic management of a 3.5-year-old male with Prader-Willi Syndrome (PWS) undergoing laparoscopic orchiopexy. The patient presented challenges typical of PWS, including potential difficult airway, obesity, and temperature regulation issues. A comprehensive preoperative evaluation and tailored anaesthetic approach were employed. Fiberoptic-guided intubation while maintaining spontaneous breathing was used for airway management, and ultrasound-guided TAP block provided pain relief. Following the uneventful intraoperative period, the patient was successfully extubated. This case highlights the importance of understanding PWS-associated complications and demonstrates that with proper preparation and technique, patients with PWS can safely undergo surgical procedures. Continued postoperative monitoring is crucial due to the risk of respiratory complications in PWS patients.
Keywords: Paediatric Anaesthesia, Syndromic Patient, Fiberoptic Intubation, Difficult Intubation, Obese Child, Prader-Willi Syndrome
Introduction
Prader-Willi syndrome is a rare genetic disorder characterized by distinct manifestations, including hypothalamic dysfunction, hypotonia, and difficulties with sucking and swallowing during infancy. In early childhood, individuals often exhibit hyperphagia, along with craniofacial anomalies, developmental delay, obstructive sleep apnea (OSA), intellectual disability, and behavioral or severe psychiatric problems [1]. Due to abnormalities of skeletal development and end-organ involvement, surgical procedures are often required in PWS patients. Scoliosis surgery, orchiopexy, adenotonsillectomy to treat OSA, ophthalmologic surgery in order to correct strabismus are surgical treatments that these patients often undergo [2]. Anaesthesia management is also challenging in such patients.
Case:
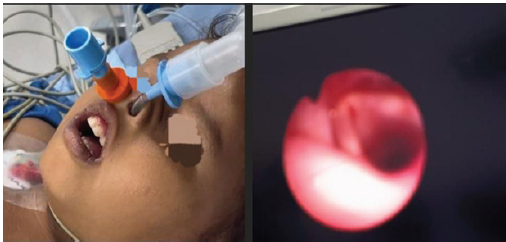
A 3.5-year-old male patient, weighing 14.6 kg, was scheduled for laparoscopic orchiopexy. The patient was born through full-term normal vaginal delivery. He did not cry immediately after birth and required NICU admission for 21 days. The patient experienced an episode of febrile convulsion, for which he received treatment that was discontinued before 1 year as advised by the paediatrician. The patient also exhibited delayed developmental milestones, being unable to walk and speak in sentences. Upon examination, the patient was found to have a small mouth, short neck, prominent buccal adiposity, central obesity and lipomatous extremities (Fig. 1). Routine investigations and vital parameters were within normal range. Following thorough preoperative evaluation, the patient was scheduled for surgery in accordance with standard ASA fasting guidelines. Standard operating theater preparation included an anaesthesia machine, difficult airway equipment with cricothyroidectomy and tracheostomy sets, oxygen supply, suction machine, forced-air warmer, and all routine and emergency anaesthesia drugs. The patient was premedicated in the preoperative room with glycopyrrolate 4 mcg/kg, fentanyl 2 mcg/kg, and midazolam 0.5 mg/kg prior to transfer to the operating theater.

Oxymetazoline nasal drops were administered in both nasal cavities. Standard monitoring was applied in the operating theater, and the patient was induced with sevoflurane in an oxygen-air mixture via mask. USG POCUS was done to mark cricothyroid membrane and to see gastric antrum. Once sedated, a red rubber nasopharyngeal airway was inserted in the right nasal cavity and sevoflurane was continuously administered through it. A fiberoptic bronchoscope was equipped with a 5 mm flexometallic uncuffed tube and inserted through the left nasal cavity. Upon achieving clear visualization of the vocal cords on the monitor, propofol at a dosage of 2 mg/kg was administered. The scope was subsequently advanced into the trachea, followed by the administration of atracurium at 0.5 mg/kg, and the tube was advanced until the carina was visible (Fig. 2 A, B). Bilateral air entry was confirmed through auscultation and end-tidal CO2 (ETCO2) monitoring prior to securing the tube. An ultrasound-guided transversus abdominis plane (TAP) block was performed using 0.25% bupivacaine at a total volume of 1 ml/kg. The intraoperative period proceeded without complications. A reversal agent was administered at the conclusion of the procedure, and the patient was subsequently extubated. The nasopharyngeal airway was maintained for 15-20 minutes in the postoperative room until the patient regained full consciousness.
Discussion:
PWS is an uncommon genetic condition characterized by obesity, hypogonadism, hypotonia and mild to moderate cognitive impairment. This disorder progresses in two phases: a hypotonic initial stage in infancy, followed by a childhood stage marked by obesity. The infant phase features poor growth, delayed developmental milestones, seizures, and light skin and eye coloration. The subsequent stage is distinguished by obesity resulting from increased appetite, along with behavioural changes, hypotonia, hypogonadism, dental caries, bone abnormalities, skin picking, and easy bruising [3].
Individuals with PWS exhibit distinctive facial features, including an elongated head, narrow face, small mouth, thin upper lip, and almond-shaped eyes [4]. Additional symptoms of PWS include non-insulin dependent diabetes, thick saliva, sleep disturbances and impaired body temperature regulation [5]. Mild to moderate cognitive impairment is often accompanied by psychological issues such as emotional instability, bouts of aggressiveness, hypersomnia and hyperphagia [6].
PWS patients present numerous challenges for anaesthesiologists. Common anticipated issues include difficult airway management and intubation, frequent respiratory infections, perioperative lung complications, impaired temperature regulation, obstructive sleep apnea (OSA), underdeveloped narrow airways, cognitive impairment, low muscle tone, and challenging intravenous access.
Both general and regional anaesthesia pose difficulties. General anaesthesia may primarily lead to airway management complications, while regional anaesthesia landmarks may be obscured due to severe obesity. Appropriate equipment for managing difficult airways should always be available for PWS patients. Considering these factors, our plan involved using a fiberoptic bronchoscope while maintaining spontaneous breathing, and administering a transversus abdominis plane (TAP) block under ultrasound guidance for pain relief. PWS patients are also susceptible to OSA and some have required reintubation during the postoperative period so postoperative monitoring is mandatory in these patients [7].
This case report presents the effective anaesthetic management of a 3.5-year-old male patient with Prader-Willi Syndrome (PWS) who underwent laparoscopic orchiopexy. The challenges associated with PWS, including potential difficult airway, obesity, and temperature regulation issues, were effectively addressed through careful preoperative evaluation and planning. The use of fiberoptic-guided intubation while maintaining spontaneous breathing proved to be a safe and effective approach for airway management. Additionally, the implementation of ultrasound-guided TAP block provided adequate pain relief, potentially reducing the need for postoperative opioids.
Conclusion:
This case emphasizes the importance of a comprehensive understanding of PWS and its associated complications when planning anaesthetic management. Syndromic paediatric patients such as those with PWS can safely undergo surgical procedures with proper preoperative assessment and preparations. Availability of difficult airway equipments and experienced anaesthesia team can provide safe anaesthesia in these patients. Continued monitoring in the postoperative period is crucial due to the risk of respiratory complications associated with PWS.
Further research and case reports on anaesthetic management of PWS patients are needed to establish best practices and improve outcomes for this challenging patient population. Anaesthesiologists should remain vigilant and prepared to address the unique needs of PWS patients throughout the perioperative period.
References
1. Butler, M. G., Miller, J. L., & Forster, J. L. (2019). Prader-Willi Syndrome – Clinical Genetics, Diagnosis and Treatment Approaches: An Update. Current Paediatric Reviews, 15(4), 207–244. https://doi.org/10.2174/1573396315666190716120925
2. Angulo, M. A., Butler, M. G., & Cataletto, M. E. (2015). Prader-Willi syndrome: a review of clinical, genetic, and endocrine findings. Journal of Endocrinological Investigation, 38(12), 1249–1263. https://doi.org/10.1007/s40618-015-0312-9
3. Dearlove, O. R., Dobson, A., & Super, M. (1998). Anaesthesia and Prader-Willi syndrome. Paediatric Anaesthesia, 8(3), 267–271. https://doi.org/10.1046/j.1460-9592.1998.00689.x
4. Gunay-Aygun, M., Schwartz, S., Heeger, S., O’Riordan, M. A., & Cassidy, S. B. (2001). The changing purpose of Prader-Willi syndrome clinical diagnostic criteria and proposed revised criteria. Paediatrics, 108(5), E92. https://doi.org/10.1542/peds.108.5.e92
5. Hertz, G., Cataletto, M., Feinsilver, S. H., & Angulo, M. (1993). Sleep and breathing patterns in patients with Prader Willi syndrome (PWS): effects of age and gender. Sleep, 16(4), 366–371. https://doi.org/10.1093/sleep/16.4.366
6. Meco, B. C., Alanoglu, Z., Cengiz, O. S., & Alkis, N. (2010). Anaesthesia for a 16-month-old patient with Prader-Willi syndrome. Journal of Anaesthesia, 24(6), 949–950. https://doi.org/10.1007/s00540-010-1005-3
7. Schlüter, B., Buschatz, D., Trowitzsch, E., Aksu, F., & Andler, W. (1997). Respiratory control in children with Prader-Willi syndrome. European Journal of Paediatrics, 156(1), 65–68. https://doi.org/10.1007/s004310050555
| How to Cite this Article: Bhagat J, Patel H, Desai P | Anaesthetic Considerations and Management Strategies for Prader- Willi Syndrome in Paediatric Surgery: A Case Report | Journal of Anaesthesia and Critical Care Case Reports | May-August 2025; 11(2): 04-06. |
(Article Full Text HTML) (Download PDF)