Vol 3 | Issue 2 | May-Aug 2017 | page: 24-26 | Y Giri, M Rahman, M Sharma.
Authors: Y Giri [1], M Rahman [1], M Sharma [1]
[1] Consultant Anesthesiologist, HAMM Hospital and RC, Hojai, Nagaon, Assam, India
Address of Correspondence
Dr. Mustafizur Rahman,
Consultant Anesthesiologist,
HAMM Hospital and RC,
Hojai, Nagaon, Assam, India – 782435.
E-mail: mustaffizur@gmail.com
Abstract
Introduction: Here we report a successful anesthetic management of a case of lung hydatid cyst (VATS) by conventional method of using double lumen tube in a rural setup with meticulous pre-operative evaluations,planning, intra-operative complication management and post-operative recovery.
Keywords: Video assisted thoracoscopic surgery (VATS), One lung ventillation (OLV), Double lumen tube (DLT)
Introduction
Lung is the second most common site for Echinococcosis granulosus infection in adults next to liver (10-30%). Surgical enucleation is the classical treatment. With the revolution of one lung ventilation (OLV) lung isolation technique, it has become very easy to perform most of the lung surgery including video-assisted thoracoscopic surgery (VATS), and lobectomies [1, 2].
Case Report
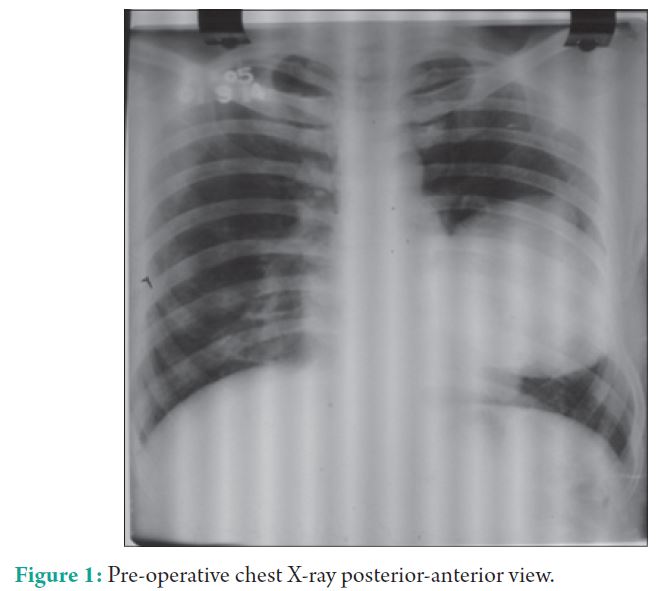
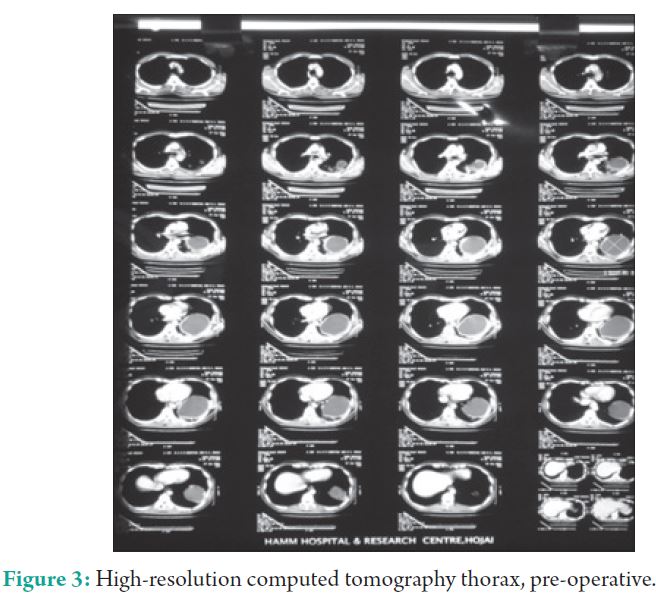
Our case report is on lung isolation technique in a giant hydatid cyst using VATS. A 40-year-old male patient, farmer by occupation, weighing 61 kg with no other comorbidities was admitted in our rural hospital with a history of progressive cough with respiratory difficulty for the past 2 years. The patient could not sleep due to intractable cough and had to take a pillow at the back for support. Pre-operative chest X-ray (Fig. 1) posterior-anterior view showed a large cystic mass in the left lung extending from 3rd to 8th rib. High-resolution computed tomography thorax (Fig. 2) showed moderately thick-walled cystic lesion (size: 11 cm × 8 cm) with small daughter cyst within and patchy consolidation of lung parenchyma around the lesion. Other investigations such as complete hemogram, liver function test, electrolyte, and electrocardiogram were normal. Ultrasound sonography abdomen performed to rule out any abdominal cyst was normal.
Case was posted for VATS under general anesthesia (GA) with OLV technique using left-sided double lumen tube (DLT). Because of limited resources and absence of fiber optic bronchoscope, we had to rely on the conventional method of DLT insertion. Case was induced with propofol and sevoflurane and vecuronium bolus was used for relaxation. After achievement of full relaxation and preoxygenation, left DLT 41F along with the stylet was introduced along the length of trachea till the proximal tracheal cuff just passed the vocal cord when it was turned 90° left, and both cuffs were inflated and checked for air entry in both lungs. Again air entry was checked separately through proximal bronchial and tracheal lumen, respectively, and both lungs were separated. Initially, the lungs were ventilated with the use of Y connector and patient was turned to the right lateral position, anesthesia was maintained with sevoflurane, nitrous oxide, and oxygen. Injection tramadol 100 mg and information. Paracetamol 1 g was used for intraoperative analgesia. Before surgical port, ventilation was switched to right lung (dependent) and left lung was deflated passively.
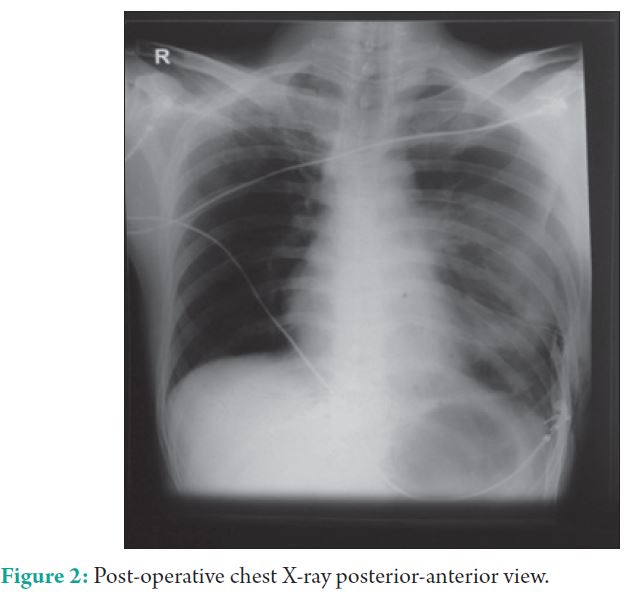
Approach for cyst was posterolateral with 10 mm camera port at midaxillary 6th intercostal space once inside the mediastinum. Though left lung was collapsed but there was still minimal leakage of gases into the left lung with each positive pressure ventillation. Since surgeon also found it difficult to operate, hence, surgery was inturrupted and double lumen tube was repositioned by slightly pushing inside but this also didn’t help. So, we introduced a suction catheter 14F through the bronchial port and attached with continuous suctioning (suction pressure upto 200 mmHg). Immediately lung was collapsed and we asked the surgeon to resume surgery. The procedure of enucleation took 30 min. Except for one episode of hypoxia managed with high-inspired oxygen concentration and positive end expiratory pressure, no other complications were encountered. There was no soiling or spillage of content either in ipsilateral or contralateral lung. Chest tube was inserted at midaxillary 6th intercostals space (site of 1st working port). At the end of surgery, left lung was inflated gradually and checked for any parenchymal air leak. After full recovery from anesthesia and with good respiratory effort, case was extubated on demand and observed for half an hour on operating table table. There were satisfactory chest excursions and bilateral air entry and oxygen saturation was well maintained. The patient had mild cough which was managed with salbutamol nebulization. The patient was shifted to intensive care unit for post-operative observation where he developed mild surgical emphysema which resolved spontaneously within 2 days. The patient was discharged on 5th post-operative day (Fig. 3) from ward after removal of chest drain with a 3-month course of albendazole.
Discussion
Double-lumen tube lung isolation technique has decreased the chance of soiling the healthy lung and allows suctioning of isolated lung and gives a good exposure for VATS, and is absolutely indicated for VATS [3, 4]. Till date, thoracotomy remains the standard surgical approach for pulmonary hydatids, so surgical experience is limited with regards to VATS, but Findikcioglu et al. showed that VATS should be the primary therapeutic choice for adults with thoracic hydatid cyst; open surgical intervention should remain optional [5]. VATS has decreased the overall hospital stay of the patients (range, 2-6 days). No recurrence or any other complications observed with mean follow-up periods of 29 months [5]. Primary case reports of VATS were in cysts of <6 cm diameter, but in our report, the longest diameter is 11 cm [6].
Conclusion
VATS for enucleation of giant uncomplicated hydatid cyst may be safely performed under GA with OLV technique using doublelumen endotracheal tube.
Acknowledgement
We would like to thank Dr. C. Islam, Senior Laparoscopic Surgeon, Dr A.H. Bhuyan, Laparoscopic Surgeon, Dr. M. Rehman, Surgeon.
References
1. Barash PG, Cullen BF, Stoelting RK. Clinical Anesthesia. 6th ed. Philadelphia, PA: Lippincott Williams & Wilkins;
2013. p. 1060-1.
2. Medycyna Praktyczna. Principles of video assisted thoracic surgery. ESTS Text Book of Thoracic Surgery. Kraków:
Medycyna Praktyczna; 2015. p. 119-22.
3. Available from: http://www.uptodate.com>contents> general principles of one lung ventilation. [Last accessed on 2017 Jun 08].
4. Available from: http://www.emedicine.Mediscape.com/ article1999993-overview. [Last accessed on 2017 Jun 08].
5. Findikcioglu A, Karadayi S, Kilic D, Hatiopoglu A. Videoassisted thoracoscopic surgery to treat hydatid disease of
the thorax in adults: Is it feasible? J Laparoendosc Adv Surg Technol A 2012;22:882-5.
6. Uchikov AP, Shipkov CD, Prisadov G. The spectrum of hydatid disease in rural cetral india: An 11 years experience. Ann Trop Med Public Health 2012;5:225-30.
| How to Cite this Article: Giri Y, Rahman M, Sharma M. VVideo-assisted thoracoscopic surgery for solitary giant hydatid cyst under general anesthesia with one lung ventilation in a rural setup: A case report. Journal of Anaesthesia and Critical Care Case Reports May-Aug 2017;3(3):24-26. |
