Vol 9 | Issue 1 | January-April 2023 | Page: 13-15 | Narayanan. K, Geeta Bhandari, Abhishek Madeshia, Shikha Singh
DOI: https://doi.org/10.13107/jaccr.2023.v09i01.213
Author: Narayanan. K [1], Geeta Bhandari [2], Abhishek Madeshia [3], Shikha Singh [4]
[1] Department of Anaesthesiology, E.S.I.C Medical College and Hospital, KK Nagar, Chennai, Tamil Nadu, India.
[2] Department of Anaesthesiology, SSJGIMSR, Almora, Uttarakhand, India.
[3] Department of Anaesthesiology, AIIMS Gorakhpur, Uttar Pradesh, India.
[4] Department of Anaesthesiology, ABVIMS, and Ram Manohar Lohia Hospital, New Delhi, India.
Address of Correspondence
Dr. Sathya Narayanan K
Assistant Professor, Department of Anaesthesiology, E.S.I.C Medical College and Hospital, KK Nagar, Chennai, Tamil Nadu, India.
E-mail: sathyavaan4444@gmail.com
Abstract
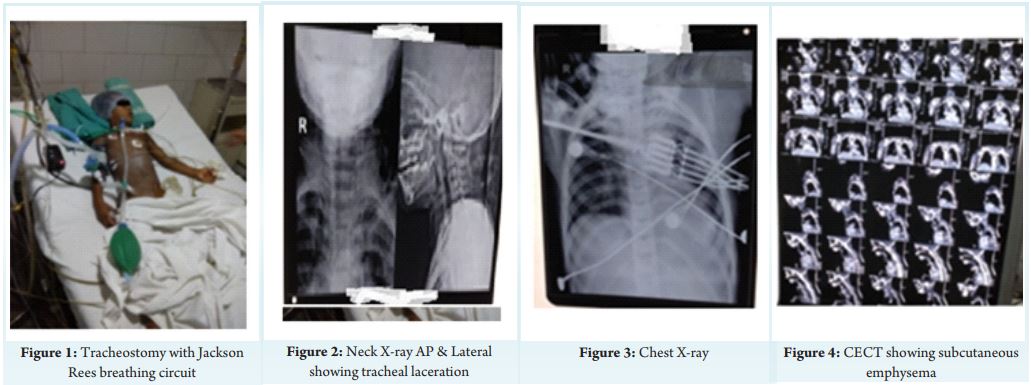
A 5-year-old girl presented to the emergency with difficulty breathing and multiple laceration all over the body after dog bite. She presented with unstable vitals and added sounds in chest, an audible inspiratory stridor and visible paradoxical breathing.
Patient was immediately shifted to intensive care unit and Bronchoscopy was performed revealing tracheal tear at 2nd and 3rd rings. CECT Neck and thorax confirmed extensive subcutaneous emphysema. Hypoxemia with uncompensated respiratory acidosis was reported in blood gas analysis. An emergency tracheostomy with size 5.0 mm was done and child was put on mechanical ventilation with appropriate settings.
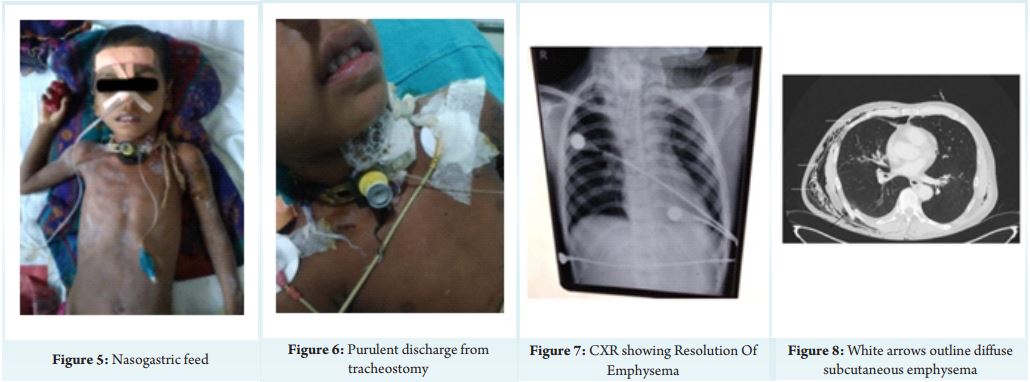
Suitable antibiotics and intravenous fluid were administered according to her weight along with rabies prophylaxis . After 5 days her chest condition improved and she was successfully weaned off.
Laryngotracheal tear following trauma is uncommon in paediatric population. Chest X-ray will reveal the presence of surgical emphysema and Computed tomography reveals the extent. Hoarseness, strider, dyspnoea are the important symptoms while surgical emphysema is often the only important sign of tracheal laceration.
Keywords: Tracheal, Laceration, Paediatric, Tracheostomy, Bubble CPAP
Introduction
Trauma management in paediatrics is a challenging task as it involves rapid efforts in resuscitation, difficulty in subjective assessment of symptoms ranging from pain management due to decreased threshold, responsiveness and dealing with emotional aspect of the parents. Tracheal laceration in pediatrics is a grave complication that follows penetrating and blunt trauma to the neck and chest [1]. It can lead to pneumomediastinum and subcutaneous emphysema, infection and aspiration. The symptoms usually depend on the amount of extravasated gas and the degree of extension of the affected areas which includes swelling, crepitus, chest pain, dyspnoea, and dysphagia [2].
Case Presentation
A 5-year-old girl weighing 12 kg presented to the emergency department with alleged history of dog bites all over the body with breathing difficulty and pain over neck region. She was presented with laceration over the neck, face, chest, left upper limb and back. On examination: Radial pulse 150/min, Blood pressure 90/45 mmHg, SPO 85% on room air, Respiratory rate 40/min and Dyspnoeic. 2Systemic examination– CNS: GCS – E4V1M6, B/L Pupils normal size and reaction, CVS: Heart sounds- normal with no murmurs, Respiratory system: Added sounds in chest, an audible inspiratory stridor and visible paradoxical breathing. Hypoxemia with uncompensated respiratory acidosis was reported in blood gas analysis. Patient was immediately shifted to intensive care unit and bronchoscopy was performed which revealed tracheal mucosal tear at 2nd and 3rd rings. Emergency tracheostomy with size 5.0 mm was done by the ENT surgeons and child was put on mechanical ventilation. The wounds were raw and multiple in number and cleansed with soap water after which sterile dressing was done and antibiotic prophylaxis with amoxicillin- clavulanate 200 mg thrice daily. Tetanus toxoid was administered less than 5 years and so it was avoided. Post exposure antirabies prophylaxis category III for 0, 3, 7 and, 28 days regimen was started intradermally in the anterolateral aspect of the thighs. Her ventilator settings were: Initially Mode- SIMV, PSV– 8 cm H2O,PEEP– 4 cm H2O, Rate– 30 cycles/min, FIO2 -100%, I:E- 1:2. CECT Neck and thorax confirmed extensive subcutaneous emphysema spreading to neck and face. Crepitus was present and milking of the air was done by making multiple nicks at the sides of face which improved her oxygenation as the emphysema improved. Gradually her arterial blood gas improved. Her ventilator stay included 6 days and she was successfully weaned and she was changed to bubble PSV CPAP mode. Initially she was kept nil per oral and intravenous fluid according to her weight was administered, but she presented with emaciated look and lost 2 kg and hence was started on nasogastric tube feeding with protein rich feeds and also antioxidants like Glutathione and Aminoacid infusions. Acetaminophen 15 mg/kg was given intravenously every 4-6 hours as needed for neck pain. She had purulent discharge from tracheostomy site and pus culture was susceptible to Acinetobacter baumanni sensitive to only Polymyxin B. Her antibiotics were revised accordingly. After 5 days, there was progressive decrease of the cervicofacial emphysema and neck pain and total resolution of the cervical emphysema and pneumomediastinum was detected in the control radiographs and arterial blood gas analysis showed adequate oxygenation. She was shifted to the paediatric ward with optimum respiratory and haemodynamic stability and was regularly followed up. Her total hospital stay was 15 days.
Discussion
Anterior neck injuries from childhood trauma occurs most commonly in sporting and adventurous activities [3]. Penetrating trauma is more common than blunt trauma [4]. The most common airway injury is the carina and main-stem bronchi followed by the trachea, and the distal bronchi [5]. The rare occurrence of tracheal injury is due to the high position of the larynx, relatively larger mandible, and the shorter neck of a child which protects the larynx and trachea airway [6]. The airway injury has caused tachypnea resulting in respiratory acidosis. Bubble CPAP (bCPAP) is most commonly followed in low resource setting and is a continuous flow device which facilitates gas exchange. It is equally efficient and is comparable to variable flow CPAP systems when used as a primary mode of respiratory support [7]. Chest X-ray will reveal the presence of surgical emphysema and computed tomography reveals the extent. Others include CT angiography and conventional angiography and duplex ultrasonography and esophagography [8]. Conservative management consisting of intensive care unit observation, humidified oxygen and antibiotic has been suggested in these patients who are haemodynamically stable and have no clinical signs of aerodigestive tract injury [9]. However, the onset of massive pneumomediastinum and pneumothorax may necessitate both tracheotomy and tube thoracostomy as initial treatment [10].Injuries from dog bites results in wound infection, cellulitis, osteomyelitis, sepsis, meningitis, endocarditis, pneumonia, and death particularly immunosupressed [11]. Wound management and initiation of antimicrobials are equally important in preventing infection. Primary closure should be avoided in limb injuries with possible risk of infection. Infected wounds presenting within 12 hours of injury are usually due to Pasteurella multocida [12].
Conclusion
As illustrated in our case, haemodynamically unstable children with subcutaneous emphysema after traumatic neck injury can be treated safely in ICU with diligent teamwork involving multiple teams and equal contributions from anaesthesiologists, paediatricicans, nurses, technicians and physiotherapists. Irrational use of drugs, frequent blood sampling must be avoided while proper nutrition and tracheostomy care should be encouraged. CT imaging and chest X-ray are used in assessing the prognosis of pneumomediastinum. Tracheal laceration in pediatrics require primary repair or tracheostomy with conservative management.
Clinical Relevance
Successful management of a tracheal injury complicating into subcutaneous emphysema and its manifestation in paediatric age group with prolonged ICU stay and treatment of tracheostomy site infection was a challenging and learning experience for the anaesthesiologists.
References
1. Marathe US, Tran LP. Pediatric neck trauma causing massive subcutaneous emphysema. Journal of Trauma and Acute Care Surgery. 2006 Aug 1;61(2):440-3.
2. Shine NP, Sader C, Coates H. Cervicofacial emphysema and pneumomediastinum following pediatric adenotonsillectomy: a rare complication. International journal of pediatric otorhinolaryngology. 2005 Nov 1;69(11):1579-82.
3. Alao T, Waseem M. Neck Trauma. [Updated 2022 Jul 4]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK470422
4. Duval EL, Geraerts SD, Brackel HJ. Management of blunt tracheal trauma in children: a case series and review of the literature. European journal of pediatrics. 2007 Jun;166(6):559-63.
5. Fette A. Trachea rupture lesion in children: the two extremes. Technology and Health Care. 2008 Jan 1;16(5):319-29.
6. Claes I, Van Schil P, Corthouts B, Jorens PG. Posterior tracheal wall laceration after blunt neck trauma in children: a case report and review of the literature. Resuscitation. 2004 Oct 1;63(1):97-102.
7. Gupta S, Donn SM. Continuous positive airway pressure: to bubble or not to bubble?. Clinics in perinatology. 2016 Dec 1;43(4):647-59.
8. Moore MA, Wallace EC, Westra SJ. The imaging of paediatric thoracic trauma. Pediatric radiology. 2009 May;39(5):485-96.
9. Sogut O, Cevik M, Boleken ME, Kaya H, Dokuzoglu MA. Pneumomediastinum and subcutaneous emphysema due to blunt neck injury: a case report and review of the literature. JPMA-Journal of the Pakistan Medical Association. 2011 Jul 1;61(7):702.
10. Andani NM, Savitri PD. Persistent secondary spontaneous pneumothorax as a complication of tuberculosis infection: a case report. Intisari Sains Medis. 2022 Feb 28;13(1):131-5.
11. Garcia VF. Animal bites and Pasturella infections. Pediatrics in review. 1997 Apr 1;18(4):127-30.
12. Morgan M, Palmer J. Dog bites. Bmj. 2007 Feb 22;334(7590):413-7.
| How to Cite this Article:Narayanan K, Bhandari G, Madeshia A, Singh S | Tracheal Laceration Due to Dog Bite in a Five Year Old Girl: The Chronicles of a Complex Case Managed Successfully | January- April 2023; 9(1): 13-15 | https://doi.org/10.13107/jaccr.2023.v09i01.213 |