Vol 4 | Issue 3 | Sep-Dec 2018 | page: 9-10| Mangal Dave.
Authors: Mangal Dave [1].
[1] Department Of Anaesthesia, Gokul hospital , Rajkot.
Address of Correspondence
Dr. Mangal Dave,
Dept. of Anaesthesia, Gokul hospital, Rajkot.
Email: mangaldave2012@gmail.com
Abstract
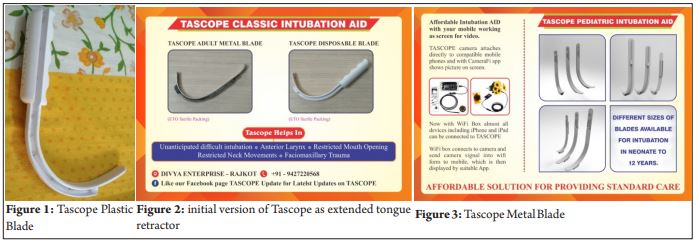
First of all thanks to Dr. Pallavi Lande and Dr. Shiv Kumar Singh Sir for inviting me to write this article. The Anaesthetist Society (TAS) is the major contributor and driving force behind successful development of TASCOPE. Well, TASCOPE is a video intubation aid to help passage of tube in difficult airways. It involves the use of endoscope or borescope camera (5.5 mm diameter HD camera) which is either connected to laptop/or even compatible mobiles or tablet, and the camera is attached on our customized TASCOPE blades. Thus, the laptop or mobile becomes screen for our intubation. Now with the help to WiFi box, even iPhone, iPad, and other noncompatible devices can also be used as screen. We have also customized channel for insertion of bougie. Then, endotracheal tube is railroaded over bougie under vision.
Tascope history
Having been working in neurotrauma center and facing difficult intubation, cervical spine injuries, and faciomaxillary trauma, we felt the definite need of a device which is affordable, easy to use, and lightweight for difficult intubation. Thus, initially fixing larger endoscope camera to extended tongue retractor, we gradually developed design with much anatomical curve and hyperacute angle for vision for difficult intubation and also found insertion of bougie initially easier than guiding styletted tube into larynx. Now, we also have design to enter even in one finger mouth opening in cases with restricted mouth opening and have developed TASCOPE PEDIA for pediatric intubation.
Intubation technique
Intubation technique remains much similar as other intubation devices such as midline insertion, pushing blade over base tongue further to visualize epiglottis, reaching up to glossoepiglottic fold, then little lift up and visualization of larynx, insertion of bougie into larynx, and then railroad tube into larynx under vision. Sometimes difficulty faced in inserting bougie, as sometime bougie might be coming out of its channel in ABS (plastic) adult blade, in which case giving proper shape (curve) to bougie and inserting it in 11 o’clock position gently will solve the issue, some friends also find the use of cut suction catheter attached over edge of blade useful. Furthermore, there can be impingement of tube bevel between arytenoids, in which tube is not getting pushed inside larynx, in these cases counterclockwise rotation of tube from 90 to 180 degrees will solve the problem.
Journey so far
I, myself, have intubated >600 difficult intubation cases with TASCOPE in the past 5 years, with 99% success, which include patient with ankylosis, fixed neck, with Philadelphia collar, and with faciomaxillary injury and fractured mandible, obese, short neck, in anticipated difficult intubation. Friends across India and abroad are using our device and find it useful in difficult intubation. At present, we have two types of adult blade (metal and ABS plastic) and three sizes pediatric blades available.
References
- Lewis G, Cantwell R, Clutton-Brock T, Cooper G, Dawson A, Drife J, et al. The Confidential Enquiry into Maternal and Child Health (CEMACH). Saving Mothers’ Lives: Reviewing Maternal Deaths to Make Motherhood Safer – 2003-2005. The 7th Report on Confidential Enquiries into Maternal Deaths in the United Kingdom. London: CEMACH; 2007.
- Sriram S, Robertson MS. Critically ill obstetric patients in Australia: A retrospective audit of 8 years’ experience in a tertiary intensive care unit. Crit Care Resusc 2008;10:120-4.
- Norwitz ER, Hsu CD, Repke JT. Acute complications of preeclampsia. Clin Obstetr Gynecol 2002;45:308-29.
- Cantwell R, Clutton-Brock T, Cooper G, Dawson A, Drife J, Garrod D, et al. Saving mothers’ lives: Reviewing maternal deaths to make motherhood safer: 2006-2008. The eighth report of the confidential enquiries into maternal deaths in the United Kingdom. BJOG 2011;118 Suppl 1:1-203.
- Wahjoeningsih S. Management of perioperative pulmonary edema in a patient with pre-eclampsia/eclampsia undergoing c-section. Folia Med Indones 2005;41:138-41.
- Easterling TR, Benedetti TJ. Pre-eclampsia. A hyperdynamic disease model. Am J Obstetr Gynecol 1989;160:1447-53.
- Dennis A, Castro C, Simmons S, Carr C, Permezel M, Royse C. Left ventricular systolic and diastolic function and structure in women with untreated pre-eclampsia. Pregnancy Hypertens 2010;1:S1-41.
- Zieleskiewicz L, Lagier D, Contargyris C, Bourgoin A, Gavage L, Martin C, et al. Lung ultrasound-guided management of acute breathlessness during pregnancy. Anaesthesia 2013;68:97-101.
- Perbet S, Constantin JM, Bolandard F, et al. Non-invasive ventilation for pulmonary edema associated with tocolytic agents during labour for a twin pregnancy. Canadian J Anesth 2008;55:769-73.
- Newstead J, von Dadelszen P, Magee LA. Pre-eclampsia and future cardiovascular risk. Expert Rev Cardiovasc Thera 2007;5:283-94.
| How to Cite this Article: Dave M. Tascope – Innovative Intubation Aid. Journal of Anaesthesia and Critical Care Case Reports Sep-Dec 2018;4(3):9-10. |

(Full Text HTML) (Download PDF)
.