Vol 7 | Issue 3 | September-December 2021 | Page: 20-22 | Poonam Darswal, Kashika Jha
DOI: 10.13107/jaccr.2021.v07i03.187
Author: Poonam Darswal [1], Kashika Jha [1]
[1] Department of Anaesthesia, QRG Health City, Faridabad, Haryana, India.
Address of Correspondence
Dr. Poonam Darswal,
QRG Health City, Faridabad, Haryana, India. 121003
E-mail: poonam.darswal@gmail.com
Successful Conduction of Mid-Humeral Fracture Surgery Under Ultrasound- Guided Supraclavicular Block an a Case of Cervical Scoliosis with Fixed Contracture Deformity Neck and Multiple Comorbidities
Abstract
Introduction: Regional anaesthesia has been proven lifesaver in many tough anaesthetic situations that demand good operative conditions yet are prone to put the patient under increased risk of post-operative complications including prolonged ICU stays even increasing overall mortality when general anaesthesia is chosen as primary anaesthesia modality. Use of ultrasound has revolutionised our approach to regional anaesthesia and many cases which would otherwise be deemed unfit for usual anatomy based approaches can now be conducted with enhanced precision and safety.
Case presentation: We present on such case in a 69-year-old male patient with multiple high-risk factors that precluded safe conduction of general anaesthesia, with the presence of cervical scoliosis with fixed contracture neck making anatomy impossible for a blind approach to brachial plexus. Even with help of ultrasound interscalene level was not accessible due to contracture. The successful supraclavicular block was made possible as we could make a clear distinction between vessels, pleura and rib at that level although the cords appeared haphazardly placed and stretched not conforming to usual anatomy at the level.
Conclusion: This case highlights the importance of regional anaesthesia under ultrasound guidance in such complex high-risk cases. As the experience with ultrasound-guided regional anaesthesia continues to grow internationally, we are on our steep learning curve appreciating the benefits and respecting the limitations of this developing technology.
Keywords: Ultrasound, Regional anesthesia, Supraclavicular block, Interscalene block
Introduction
The supraclavicular block has many advantages that make it an attractive option for anaesthesia or analgesia in upper limb surgeries. Besides being compactly placed and superficially located at this level, it usually doesn’t require special limb positioning [1, 2]. The use of ultrasonography further enhances safety and significantly reduces the potential of pneumothorax or Hemi-diaphragmatic palsy [3]. These potential problems could add to the burden of post-op respiratory complications in already compromised patients with underlying COPD or Asthma, and jeopardize their path to recovery [4].However, at times it is very difficult to satisfactorily locate the brachial plexus clusters in some people as was seen in our case where ultrasound helped in providing successful supraclavicular block for surgery. It allows for important landmarks to be seen in real-time and block can be given based on a normal anatomical correlation of brachial plexus to them.
Case Report
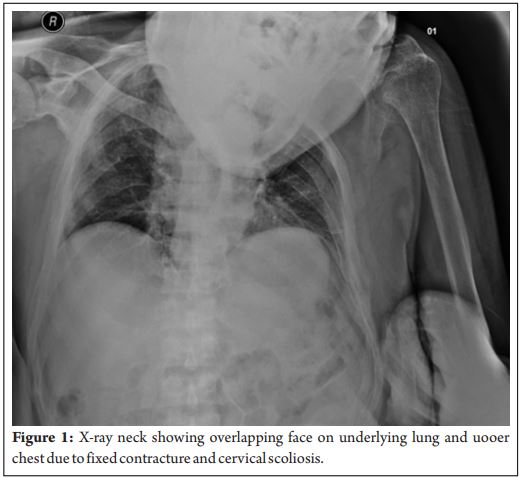
Our patient was a 69-year-old gentleman with fracture mid-humerus on the left side. He had a history of hypertension, COPD, cerebrovascular accident (2007) with residual quadriparesis. He was bedridden since 2007 and had developed fixed contractures in the left arm and left lower limb with a scoliotic deformity in the cervical region.On examination, the patient had a resting pulse rate of 110/min, BP of 140/80 mm hg, RR of 28-30/min and saturation of 94% room air. The patient had a bilateral wheeze and ronchi, more prominent in lower lung zones. Because of a very poor effort and co-operation, PFTs could not be done. Respiratory optimization was done with bronchodilators in form of nebulizer levolin/foracort and intravenous deriphylline by our respiratory team. In the fractured limb, he had a fixed flexion abnormality at the elbow. His sensory powers were normal while the motor component could not be accurately assessed due to the contracture. His 2D echo was normal and ECG showed no major changes.His right lower limb had swelling and calf tenderness. The patient family refused for Doppler assessment for ruling out DVT.Airway examination revealed a grossly limited extension and flexion as the neck was fixed in flexion and rotation towards the left side due to scoliosis of the cervical spine (Fig.1).The patient had very poor dental hygiene with multiple missing and carious teeth. The safe conduction of general anaesthesia would have been a potential threat to an uneventful postoperative recovery of this patient with a high risk of perioperative pulmonary complications including bronchospasm/laryngospasm/pneumonia, need for prolonged mechanical ventilation among others.It was a challenging scenario that we desired to make less threatening for the patient by opting for a regional anaesthesia technique. Presence of cervical scoliosis and neck-contractures made any approach to the brachial plexus very difficult to attempt. The supraclavicular block was selected as it provides good surgical conditions for upper arm surgery as compared to axillary or infraclavicular blocks with low the risk of hemi-diaphragmatic palsy seen in interscalene block.Ultrasound guidance proved to be a boon in this case where typical landmarks were not discernable at all. The nerve roots appeared haphazardly placed and the plexus failed to conform to the expected grape-bunch appearance or superolateral placement with respect to the arterial pulsations. The block was given keeping in mind the normal anatomical relations of the plexus to the pulsations of the artery, pleura and the first rib which were identifiable above the clavicle. Although with some difficulty.A total of 20 ml 0.5% bupivacaine was injected below and on both sides of the artery. The patient tolerated the procedure well and surgery took 1.5 hours to complete. O support via nasal prongs was provided 2throughout the surgery. A propped up position was maintained and constant verbal contact was maintained with the patient with repeated assurances to allay his anxiety. The diaphragm movements, breathing pattern, respiratory rate and SpO was continuously monitored, and the patient did not show any 2signs of respiratory deterioration throughout the procedure. ECG, NIBP measurements were done as per ASA standards. He did not report any deterioration in sensation or motor power in his limb till 48 hours post-surgery. We maintained constant communication with the nursing team and his family regarding the same.Unfortunately, the patient party did not permit filming or photography of any kind during or after the procedure which would have been an immense help in compiling and understanding of this manuscript. Fully informed consent was taken for case reporting.The patient had an uneventful hospital stay and was discharged on day 2 of surgery.
Discussion
The indispensable support from the use of ultrasound in modern anaesthesia practice is now a widely accepted norm with reported success rates between 78% and 95%[5, 6, 7]. Using ultrasound has not only made routine anaesthesia practice safer but added to the armamentarium of the anaesthetist in difficult scenarios. It helps in delineating the underlying anatomy, helping in differentiating different tissues particularly aiding in safeguarding against accidental vessel punctures. In a case series of 105 patients by Dae Geun Jeon, and Won Il Kim, it was found that 13 cases (12.4%) had brachial plexus anatomy that was vague or not visible on the ultrasound image and they injected LA based on the normal anatomy like in our case and had a success rate of 84.6% against rest of group rate of 98.9% [8]. It was believed that injecting LA lateral or superior lateral to the subclavian artery could reach the brachial plexus as guided by the normal anatomical pattern of location of plexus around the artery at the level of the first rib. Our case had a peculiar problem of being at very high risk for a general anaesthesia exposure due to presence of multiple systemic comorbidities and the simultaneous presence of neck contracture with cervical scoliosis that made complicated safe delivery of regional as well. A poor respiratory reserve as seen in this case puts the perioperative course at high risk of post-op respiratory complications [4]. Attempting a supraclavicular block based on anatomical landmarks only would have put this patient at high risk of incomplete/failed block, accidental vascular/pleural puncture, need for high volume block with high chances of systemic toxicity and phrenic nerve block due to difficult anatomy.A supraclavicular block although has many advantages, yet it has potential for some serious complications, most important to our case was a fear of dyspnea due to phrenic nerve palsy or pneumothorax due to accidental pleural puncture [1, 2]. Studies have reported a 30-50% incidence of hemi-diaphragmatic palsy with a supraclavicular block but without any effect on the FVC [9, 10]. This makes it a favourable approach in cases where further respiratory compromise is not is tolerable. The published incidence of pneumothorax varies from 0.5% to 6% in the classical supraclavicular approach with paresthesia for nerve localization [1, 2]. Ultrasound guidance is believed to decrease the incidence of pneumothorax during a supraclavicular brachial plexus block [5]. C. Kakzu reported a 0% incidence of pneumothorax in their 5-year study of USG guided supraclavicular blocks [11]. The high incidence of phrenic nerve palsy (100%) in the interscalene approach accompanied by a 25% decrease in the forced vital capacity (FVC) makes this approach unfavourable for such cases [12].With a detailed discussion of all risks involved in general as well as regional anaesthesia to the patient party and surgical team, it was decided to attempt supraclavicular block with ultrasound guidance. As expected the anatomy was grossly distorted with stretched and haphazardly placed cords at this level lacking a clear bunch of grape anatomy or arterial relationship. Keeping pleura, first rib and arterial pulsations as landmark approximately 20 ml of 0.5% bupivacaine was injected slowly around the artery in 2 to 3 ml aliquots following negative aspiration. A good motor and sensory block were obtained in 20 minutes and surgery was completed uneventfully. The presence of ultrasound in the scenario markedly improved the post-op course wherein patient could be discharged to home on 2nd post-op day.
Conclusion
This case highlights the importance of regional anaesthesia in such complex cases and the importance of maintaining transparent communication with the patient party and surgical team.
Clinical Relevance
As the experience with ultrasound-guided regional anaesthesia continues to grow internationally, we are on our steep learning curve appreciating the benefits and respecting the limitations of this developing technology.
References
1. Fleisher LA, Johns RA, Savarese JJ, Wiener-Kronish JP, Young WL. Miller’s Anesthesia. 6th ed. Philadelphia, Churchill-Livingstone. 2005, p 1690.
2. Morgan GE, Mikhail MS, Murray MJ. Clinical Anesthesiology. 4th ed. New York, Lange Medical Books/McGraw-Hill Medical Publishing Division. 2006, pp 332-3.
3. Kapral S, Krafft P, Eibenberger K. Ultrasound-guided supraclavicular approach for regional anesthesia of the brachial plexus. Anesth Analg 1994; 78: 507-13.
4. Numata et al. BMC Pulm Med (2018) 18:4 DOI 10.1186/s12890-017-0570-8.
5. Williams SR, Chouinard P, Arcand G, Harris P, Ruel M, Boudreault D, et al. Ultrasound guidance speeds execution and improves the quality of supraclavicular block. Anesth Analg 2003; 97: 1518-23.
6. Chan VW, Perlas A, Raw R, Odukoya O. Ultrasound-guided supraclavicular brachial plexus block. Anesth Analg 2003; 97: 15147.
7. Tsui BC, Doyle K, Chu K, Pillay J, Dillane D. Case series: ultrasound-guided supraclavicular block using a curvilinear probe in 104 day case hand surgery patients. Can J Anaesth 2009; 56: 46-51.
8. Dae Geun Jeon, and Won Il Kim. Cases series: ultrasound-guided supraclavicular block in 105 patients. Korean J Anesthesiol 2010 Mar; 58(3): 267-271 DOI: 10.4097/kjae.2010.58.3.267
9. Farrar MD, Scheybani M, Nolte H. Upper extremity block, effectiveness and complications. Reg Anesth 1981; 6: 133-4.
10. Neal JM, Moore JM, Kopacz DJ, Liu SS, Kramer DJ, Plorde JJ. Quantitative analysis of respiratory, motor, and sensory function after supraclavicular block. Anesth Analg 1998; 86: 1239-44. .
11. Urmey WF, Talts KH, Sharrock NE. One hundred percent incidence of hemidiaphragmatic paresis associated with interscalene brachial plexus anesthesia as diagnosed by ultrasonography. Anesth Analg 1991; 72: 498-503.
12. C. Kakazu, V. Tokhner, J. Li, R. Ou, E. Simmons. In the new era of ultrasound guidance: is pneumothorax from supraclavicular block a rare complication of the past? BJA 2014;113(1): 190–191.
| How to Cite this Article: Darswal P, Jha K | Successful Conduction of Mid-Humeral Fracture Surgery Under Ultrasound-Guided Supraclavicular Block an a Case of Cervical Scoliosis with Fixed Contracture Deformity Neck and Multiple Comorbidities | Journal of Anaesthesia and Critical Care Case Reports | September-December 2021; 7(3): 20-22. |