Vol 9 | Issue 3 | September-December 2023 | Page: 18-20 | Mohamad Ibrahim Ayoub, Cesar Padilla, Justo Gonzalez, Husien Taleb, Elie Geara, Adeeb Oweidat
DOI: https://doi.org/10.13107/jaccr.2023.v09.i03.226
Submitted: 11/05/2023; Accepted: 11/07/2023; Published: 10/09/2023
Author: Mohamad Ibrahim Ayoub [1], Cesar Padilla [2], Justo Gonzalez [3], Husien Taleb [3], Elie Geara [1], Adeeb Oweidat [4]
[1] Department of Anaesthesiology, NYU Grossman School of Medicine, NYU Langone Health, NY.
[2] Department of Anaesthesiology, Stanford Hospital, CA.
[3] Department of Anaesthesiology, Cleveland Clinic, OH.
[4] Department of Anaesthesiology, University of Iowa Hospitals & Clinics, Lowa City, US.
Address of Correspondence
Dr. Mohamad Ibrahim Ayoub,
Department of Anaesthesiology, NYU Grossman School of Medicine, NYU Langone Health, NY.
E-mail: ayoub.mohamad.89@gmail.com
Abstract
We describe a case of preeclampsia where lung ultrasonography facilitated the diagnosis of pulmonary edema while also showing real-time resolution of B-lines after diuresis. The diagnostic accuracy of B-line clearance using lung ultrasonography across diverse patient populations (heart failure, renal failure) holds promise for use in the obstetric patient population. To our knowledge this is the first report which shows real-time resolution of B-lines using lung ultrasonography in a pregnant patient with preeclampsia associated pulmonary edema. Given the established validity of this tool, we believe lung ultrasonography holds promise in the management of critically ill obstetric patients.
Keywords: Preeclampsia, TTE (transthoracic echocardiography), POCUS (point-of-care ultrasonography), FRC (functional residual capacity), B-lines, A-lines
Introduction
Preeclampsia is a multiorgan disease which is characterized by hypertension and proteinuria in pregnancy after 20 weeks of gestation and up to six weeks in the postpartum period [1, 2]. In the United States, additional expenditure from preeclampsia is over 2 billion dollars when accounting for both maternal and neonatal related complications [3]. Preeclampsia is estimated to affect 2-8% of all pregnancies worldwide, however the incidence of preeclampsia in patients with a history of chronic hypertension has been reported as high as 17-25% [4].
The incidence of cardiovascular and pulmonary complications detected by lung ultrasonography (point of care ultrasonography) have been reported to occur in 67% of patients with late onset preeclampsia with severe features. These findings include pulmonary edema (pulmonary interstitial syndrome), diastolic dysfunction and systolic dysfunction which occur in 24%, 33% and 10% of cases [5].
Point-of-care ultrasound (POCUS) therefore becomes a valuable tool in providing clinicians with real time data, helping guide clinical management. Although the utility of POCUS is validated in other clinical settings (emergency and intensive care setting), there is little data in regard to outcomes related to POCUS in pregnant patients.
We describe a case of a 23-year-old pregnant patient at 30 weeks and 1 day of gestation admitted for the management of preeclampsia with severe features. Lung ultrasonography facilitated the diagnosis of acute pulmonary edema while also showing real-time resolution after diuresis. To our knowledge this is the first published case which shows real-time ultrasonographic resolution of pulmonary edema using lung ultrasonography in a pregnant patient with preeclampsia associated pulmonary edema after diuresis. This case highlights the need for further research and validation of this tool in the obstetric population. HIPAA authorization has been obtained from the patient. All author have followed the appropriate EQUATOR guidelines.
Case Description
A 23-year-old female at 30 weeks and 1 day gestation was admitted to the labor and delivery unit due to an acute rise in blood pressure and new onset headache. The patient’s past medical history is significant for chronic hypertension (pre-pregnancy), asthma, supraventricular tachycardia (remote history of arrhythmias) and morbid obesity (150 kg, BMI 56). The patient’s pregnancy was otherwise unremarkable for acute events. As an outpatient she was managed with labetalol (100 mg BID) at home with good blood pressure control.
On day 2 of the patient’s hospitalization, she required increasing doses of labetalol (400 mg TID) and the addition of a second antihypertensive (Nifedipine 20 mg doses as needed) for progressively increasing blood pressure measurements. The patient’s respiratory status remained stable throughout this time and she remained on room air with a normal oxygen saturation (>98% SpO2).
On day 3 of hospitalization the patient’s blood pressure continued to rise (BP 190/107, 170/90, 180/95, 15 minutes apart) while she developed new onset shortness of breath with an acute increase in oxygen requirement to 10 liters of oxygen (delivered via a facemask). During this time fetal heart tracing worsened and was noted to be category II with minimal variability.
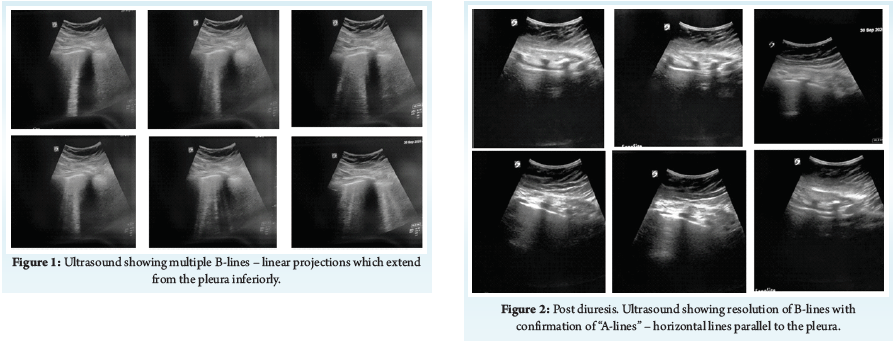
At this time the patient received 3 additional doses of intravenous labetalol (20 mg, 40mg and 80 mg) with little control of blood pressure; (BP 150/100) after treatment. Lung ultrasound was performed at this time with a transabdominal curvilinear probe (Sonosite, 8-5 MHz) which showed a bilateral pattern of “B Lines” with 4 total positive zones (2 positive zones bilaterally with >3 B Lines) based on established protocols for diagnosing interstitial syndrome (Figure 1) .
A limited point of care cardiac ultrasound was also performed which showed normal biventricular function (fractional shortening >21%) with grossly normal cardiac ultrasound findings (no evidence of regional wall motion abnormality or pericardial tamponade). After TTE and lung ultrasound assessment and a multidisciplinary discussion with the obstetric, maternal fetal medicine and anesthesiology teams, it was determined to diurese the patient (Furosemide (40 mg IV) in preparation for an urgent delivery via a cesarean section (due to worsening fetal heart tracing and inability to continuously monitor fetal heart rate due to body habitus).
The patient’s urine output was 1.2 liters within 1 hour of diuretic administration. This coincided with an improvement in oxygenation (oxygen weaned to 3 liters via nasal cannula) and symptomatic improvement in patient’s respiratory effort (Figure 3).
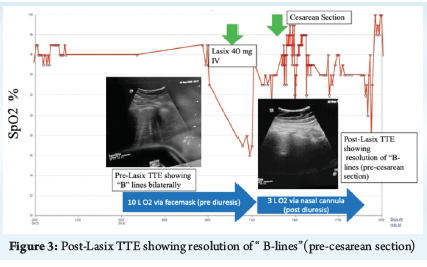
Approximately 1 hour later the patient was transported to the operating room for a cesarean section where a repeat POCUS exam (lung ultrasound) was performed which showed resolution of B-lines bilaterally with A lines present (Figure 2). A combined spinal epidural (12 mg of 0.75% hyperbaric bupivacaine, 20 mcg fentanyl, 100 mcg morphine) was then performed and the patient was placed in a 15-degree left uterine tilt position. The obstetrics team proceeded with a cesarean delivery via a primary low transverse cesarean section. A 1.2 kg male was born with Apgar scores of 7 and 8, respectively. The patient was maintained on 3 liters of oxygen (via nasal cannula) for the duration of the case with stable hemodynamics. In the post anesthesia care unit, a repeat TTE was performed which confirmed absence of B lines bilaterally (A-lines). The patient’s recovery was uneventful and the patient was weaned off oxygen on post-operative day 1. The patient was successfully discharged on day 6 of hospitalization with an antihypertensive regimen of labetalol.
Discussion
Ultrasonography has shown validity in diagnosing cardiopulmonary disorders and pulmonary edema. The diagnostic accuracy is superior when compared to standard chest film technology (X-ray). The sensitivity and specificity of lung ultrasonography in identifying pulmonary edema is 86% and 97%, respectively [6]. The pattern of “B lines”, or vertical projections which originate at the level of the pleura and extend inferiorly, is an ultrasonographic pattern which occurs due to the acoustic impendence values of water and air, which causes ultrasound beams to create vertical patterns [7].
Standardization for ultrasonographic patterns of interstitial syndrome has created expert consensus for the diagnostic threshold of B-lines and interstitial syndrome. The presence of 3 or more B lines in at least 2 bilateral lung zones is considered a positive finding for interstitial syndrome [8]. In patients with cardiogenic shock, the number of B-lines has also been found to correlate with the degree of pulmonary edema, measured as extravascular lung water (EVLW) [9].
In patients with pulmonary edema from heart failure, clearance of B-lines has strongly correlated with medical and clinical recovery, such as improvement in chest radiography and lower natriuretic peptide levels [10]. Real time B-line resolution has also been shown in patients undergoing hemodialysis, with progressive clearance of B lines as fluid is removed [11]. The diagnostic utility of lung ultrasound in pregnancy and pregnancy associated disorders is limited to few studies. Recently, Ortner et al. demonstrated that pulmonary edema occurs in 24% of pregnant patients with late onset preeclampsia with severe features [5].
Sonographic resolution of pulmonary edema utilizing lung ultrasonography in a pregnant patient with preeclampsia has not been reported. To our knowledge this is the first report showing real time resolution of B-lines after diuresis in a patient with preeclampsia induced pulmonary edema. Our case report highlights the facile nature of utilizing lung ultrasonography in a pregnant patient while contributing vital data which directly contributed to critical medical management. The feasibility and non-invasive nature of lung ultrasonography makes this a valuable tool in the acute medical setting. In our patient the resolution of B-lines was associated with evidence of clinical improvement. The patient’s oxygen requirement was significantly reduced from 10 liters via facemask to 3 liters via nasal cannula in a short period (1 hour) after diuretic administration (Figure 3).
The medical stabilization of our patient was prudent and allowed for the safe delivery of neuraxial anesthesia. The loss of accessory muscles of respiration, notably intercostal muscles, can predispose an already respiratory compromised patient to hypoxia [12]. Moreover, due to physiologic changes of pregnancy, the supine position compromises functional residual capacity (FRC), worsening hypoxia in the supine position. This reduction in oxygenation reserve is exacerbated by our patient’s body habitus (morbid obesity), further compromising FRC is in the supine position, predisposing to hypoxia [13].
Conclusion
Our case report is showing real time clearance of B-lines in a pregnant patient with pulmonary edema from preeclampsia. The reliability and diagnostic accuracy of B-line clearance using lung ultrasonography is established across diverse patient populations (heart failure, renal failure) and holds promise in the obstetric patient population. More evidence is needed to assess the validity of lung ultrasonography and associated pattern changes (B-line clearance) in pregnancy. Given the previously established diagnostic validity of this tool, we believe TTE (lung ultrasonography) holds tremendous promise in the management of critically ill obstetric patients.
Abbreviations: TTE (transthoracic echocardiography), POCUS (point-of-care ultrasonography), FRC (functional residual capacity).
References
1. Gestational Hypertension and Preeclampsia. Practice Bulletin. American College of Obstetricians and Gynecologists. June 2020. https://www.acog.org/clinical/clinical-guidance/practice-bulletin/articles/2020/06/gestational-hypertension-and-preeclampsia
2. Steegers EA, von Dadelszen P, Duvekot JJ, Pijnenborg R. Pre-eclampsia. Lancet 2010;376:631–44. (Level III).
3. Stevens W, Shih T, Incerti D, Ton TGN, Lee HC, Peneva D, et al. Short-term costs of preeclampsia to the United States health care system. Am J Obstet Gynecol 2017; 217:237–48.e16. (Level III).
4. Seely EW, Ecker J. Chronic hypertension in pregnancy. Circulation. 2014 Mar 18;129(11):1254-61.
5. Ortner CM, Krishnamoorthy V, Neethling E, Flint M, Swanevelder JL, Lombard C, Fawcus S, Dyer RA. Point-of-Care Ultrasound Abnormalities in Late-Onset Severe Preeclampsia: Prevalence and Association With Serum Albumin and Brain Natriuretic Peptide. Anesth Analg. 2019 Jun;128(6):1208-1216.
6. Volpicelli G, Melniker LA, Cardinale L, Lamorte A, Frascisco MF. Lung ultrasound in diagnosing and monitoring pulmonary interstitial fluid. Radiol Med. 2013 Mar;118(2):196-205. doi: 10.1007/s11547-012-0852-4. Epub 2012 Jun 28. PMID: 22744356.
7. Soldati G, Copetti R, Sher S (2009) Sonographic interstitial syndrome: the sound of lung water. J Ultrasound Med 28:163–174.
8. Liteplo AS, Marill KA, Villen T, et al. Emergency thoracic ultrasound in the differentiation of the etiology of shortness of breath (ETUDES): sonographic B‐lines and N‐terminal pro‐brain‐type natriuretic peptide in diagnosing congestive heart failure. Acad Emerg Med 2009;16:201–10.
9. Jambrik Z, Monti S, Coppola V et al (2004) Usefulness of ultrasound lung comets as a nonradiologic sign of extravascular lung water. Am J Cardiol 93:1265–1270.
10. 41. Volpicelli G, Caramello V, Cardinale L et al (2008) Bedside ultrasound of the lung for the monitoring of acute decompensated heart failure. Am J Emerg Med 26:585–591.
11. Noble VE, Murray AF, Capp R et al (2009) Ultrasound assessment for extravascular lung water in patients undergoing hemodialysis. Time course for resolution. Chest 135:1433–1439.
12. David O. Warner, Mark A. Warner, Erik L. Ritman; Human Chest Wall Function during Epidural Anesthesia. Anesthesiology 1996; 85:761–773.
13. Taylor CR, Dominguez JE, Habib AS. Obesity And Obstetric Anesthesia: Current Insights. Local Reg Anesth. 2019;12:111-124. Published 2019 Nov 18.
| How to Cite this Article: Ayoub MI, Padilla C, Gonzalez J, Taleb H, Geara E, Oweidat A. Sonographic Resolution of B-Lines after Diuresis in a Pregnant Patient with Preeclampsia Associated Pulmonary Edema. Journal of Anaesthesia and Critical Care Case Reports. September-December 2023; 9(3): 18-20. https://doi.org/10.13107/jaccr.2023.v09.i03.226 |
(Full Text HTML) (Download PDF)