Vol 4 | Issue 1 | Jan-Apr 2018 | page: 31-34 | Ritesh Roy, Shiv Kumar Singh, Gaurav Agarwal, Chandrasekhar Pradhan
Authors: Ritesh Roy [1], Shiv Kumar Singh [2], Gaurav Agarwal [1], Chandrasekhar Pradhan [1]
[1] Consultant Anesthesiologist, CARE Hospitals,
Chandrasekharpur, Bhubaneswar, Odisha, India,
[2] Consultant Anaesthesiologist, Royal Liverpool University Hospitals, Liverpool, UK.
Address of Correspondence
Dr. Gaurav Agarwal,
1510/B, Sector 6, CDA,
Cuttack– 753014, Odisha, India;
E-mail: dr.agarwalgaurav@gmail.com
Abstract
Introduction: Thoracic epidural and paravertebral blocks, the gold standard for post-operative analgesia for chest wall surgeries have a high incidence of complications and adverse effects. The pectoralis (PEC) blocks, first described by Blanco et al., have been proven to provide good analgesia postoperatively for breast surgeries, wide pectoral dissections, upper chest injuries, pacemaker insertions, port-a-cath placements, and intercostal chest drains. To widen the scope of this simple and useful analgesia technique, which mandates the availability of ultrasound machine and indepth knowledge of the sonoanatomy of the area, we are describing the conduct of PEC-I block using peripheral nerve stimulator, which is easily available to most anesthetists.
Description of the Technique: Medial and lateral pectoral nerves (LPNs) are motor nerves originating in the brachial plexus innervate the pectoral muscles. The LPN runs in between pectoralis major and pectoralis minor muscle alongside the pectoral branch of thoracoacromial artery and supplies the pectoralis major muscle. The LPN communicates with the medial pectoral nerve and is known to carry nociceptive and proprioceptive fibers. The patient lies in a supine position with ipsilateral arm slightly abducted. The injection point is the intersection of a line drawn from the angle of Louis (2nd rib) and the anterior axillary line. After local infiltration of the skin with 1% lignocaine, a 50 mm insulated nerve stimulator needle with syringe filled with local anesthetic attached to the extension tubing is inserted perpendicular to the skin. The peripheral nerve stimulators (PNS)are initially set at 1.0–1.5 mA current, 0.1ms duration, and frequency of 1Hz. The needle is slowly advanced till the pectoralis muscle contractions is noted, with a current threshold of 0.3–0.5 mA. Persistence of contraction of pectoralis muscle at this level confirms the needle placement at the target site. The LA is then slowly injected in increments with frequent negative aspirations.
Discussion: An increasing numbers of breast surgeries warrant better post-operative analgesia techniques, with fewer complications.Thoracic epidural analgesia, thoracic paravertebral blocks (TPVB), and intercostal nerve blocks have all been very effective for such surgeries but, are associated with complications such as epidural hemat omas, nerve injuries, pneumothorax,and hypotension. Analgesia technique like TPVB was unreliable with a single injection, and pectoral nerves were still spared producing inadequate analgesia of the chest wall and needed post-operative monitoring. The pectoralis block (PEC block), a novel technique, was described by Blanco et al. in 2011 using ultrasound and was easy, reliable, and associated with fewer complications. Peripheral nerve stimulator for such an easy and superficial block increases the utilization and benefits wider population. We have described the use of PNS for PEC-I block that can be used as a sole analgesia technique for breast implant insertion, pacemaker implantation, porta-cath insertion, ICD insertions or removals, and pectoralis muscle flaps. The PEC-I block can be further combined with PNS guided serratus anterior plane block to achieve excellent analgesia of the chest wall for surgeries.
Conclusion: The PEC-I block along with PEC-II or SA plane block has a high success rate and minimal incidence of complications and provides a consistent and reliable block for hemithorax analgesia. In this article, we describe PEC-I block using PNS which is easily available to most anesthetist,unlike US machines which are available only to very few. PNS guided PEC-I block will increase the scope of this superficial, easy, and reliable block.
Keywords: Pectoralis blocks, chest wall blocks, pectoralis-I, pectoralis-II, peripheral nervous system, peripheral nervous system guided chest wall block.
Introduction
Chest wall surgeries especially breast surgeries are commonly performed as daycare surgeries in most centers around the world. Even though these surgeries are superficial, they are associated with significant post-operative pain [1,2]. The gold standard for post-operative analgesia for surgeries is thoracic epidural analgesia (TEA) or thoracic paravertebral blocks (TPVB) [3,4] Both TEA and TPVB are associated with significant complications and adverse effects and thus make them unsuitable for day-care surgeries. In 2011, Blanco first described a superficial and novel analgesia technique, pectoralis (PEC) block, for such cases in correspondence to anesthesia. [5,6] In the following year, he published a detailed description of the ultrasound-guided technique for PEC and modified PEC or PEC-II blocks [7]. The PEC blocks have proven to provide excellent analgesia postoperatively for breast surgeries, [5,6,7] wide pectoral dissections, [8,9] upper chest injuries, pacemaker insertions, port-a-cath placements, and insertion, and removal of intercostal chest drains [10]. The PEC-I block is described to be an easy and reliable superficial block but mandates the availability of ultrasound machine and in-depth knowledge of the sonoanatomy of the area. To widen the scope of this simple and useful analgesia technique, we describe the use of the peripheral nerve stimulators (PNS), easily available to most anesthetist, to perform the PEC-I block.
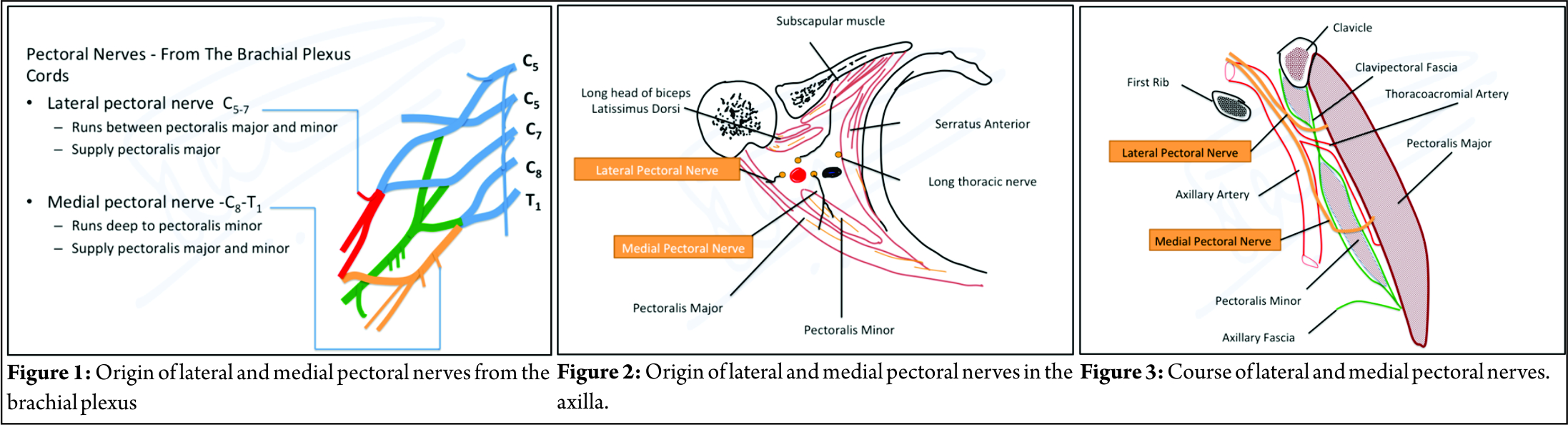
Anatomy Relevant to the PEC-I Block Medial and lateral pectoral nerves (LPNs) that take origin in the brachial plexus innervate the pectoral muscles. Both these nerves are motor; theLPN arises from the C5,6,7 nerve roots and the medial pectoral nerve (MPN) from C8 and T1(Fig.1 and 2). The LPN runs in between pectoralis major and pectoralis minor muscle alongside the pectoral branch of thoracoacromial artery and supplies the pectoralis major muscle (Fig.2). The LPN communicates with the medial pectoral nerve and is known to carry nociceptive and proprioceptive fibers. The medial pectoral nerve is the smaller branch of the two; it originates from the brachial plexus posterior to the axillary artery and then gives anumber of branches as it pierces the pectoralis minor and supplies the deeper part of thepectoralis major, the sternocostal fibers (Fig.3) [11,12].
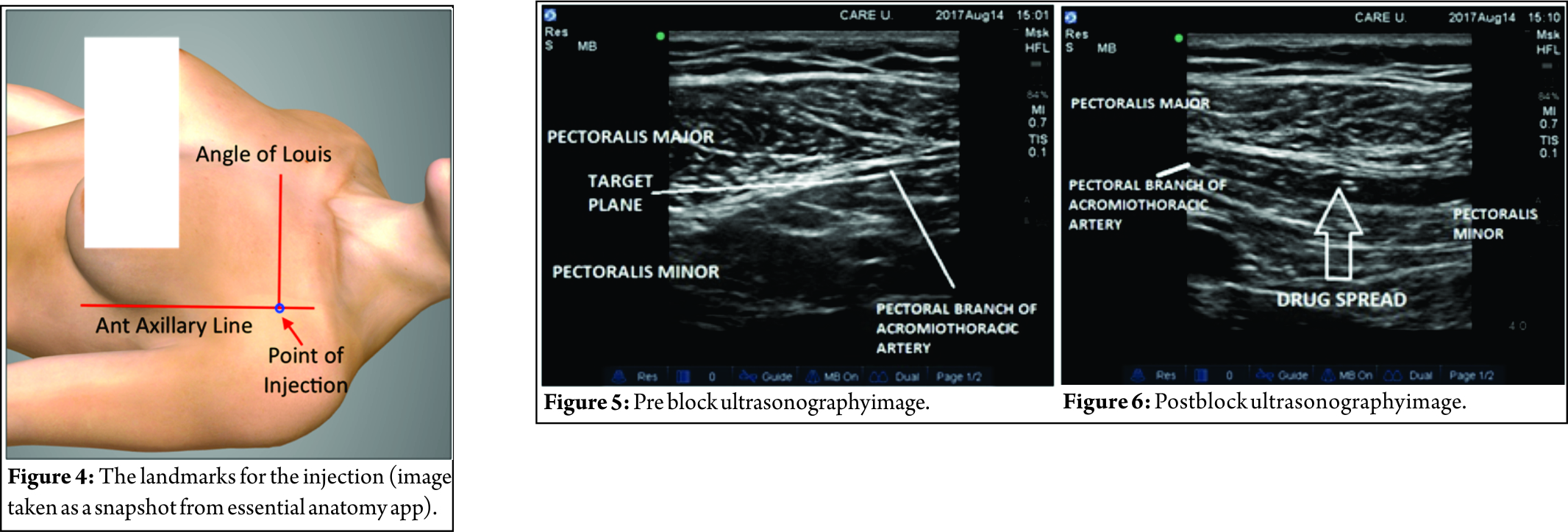
Description of the Technique The PEC-I block done by PNS technique requires the patient to lie in a supine position with ipsilateral arm slightly abducted. The landmark for the block is a point where a line drawn from the angle of Louis (2nd rib) joins the anterior axillary line. This point of intersection is the needle insertion point (Fig. 4). The block is done with a 50 mm insulated nerve stimulator needle with syringe filled with local anesthetic (LA) attached to the extension tubing. After local infiltration of the skin with 1% Lignocaine, the needle is inserted perpendicular to theskin, at the landmark described above. The PNS is initially set at 1.0–1.5 mA current, 0.1ms duration,and frequency of 1Hz. The needle is slowly advanced till the pectoralis muscle contractions is noted. The needle is kept at this depth and current is gradually reduced to 0.3–0.5 mA. Persistence of contraction of pectoralis muscle at this level confirms the needle placement at the target site. The LA is then slowly injected in increments with frequent negative aspirations.
Discussion
An increasing numbers of breast surgeries being done both for therapy of breast cancer as well as cosmetic reasons warrant better post-operative analgesia techniques that are associated with fewer complications and reduce the length of hospital stay or allow for same-day discharge. Regional anesthesia techniques such as TEA, TPVB, and intercostal nerve blocks (ICNB) have all proven to be the very effective for such surgeries [1,2] but are associated with complications such as epidural hematomas, nerve injuries, pneumothorax, and hypotension [13,14,15,16]. These analgesia techniques need to be mostly done before administration of general anesthesia to recognize and reduce the incidence of the associated complications. Analgesia technique like TPVB, when used in day-care setting, was found to be unreliable with a single injection [17]. Multiple injections were found to be more effective [18] but pectoral nerves were still spared producing inadequate analgesia of the chest wall, and post-operative monitoring was required making it unsuitable for same day discharge from the hospital. To overcome this limitation a novel technique for chest wall blocks, the pectoralis block (PEC block) was described by Blanco in 2011 and then in 2012 in an article. He described an intermyofascial injection of LA between the pectoralis major and minor muscles to block the pectoral nerves. This approach using ultrasound was novel, superficial than TEA, TPVB, or ICNB and easy to use [8,9]. The PEC block done under US guidance has alower risk of intravascular injection than TPVB. The possibility of injection into the pectoral branch of the acromiothoracic artery remains;however, these complications can be easily avoided with proper ultrasound training and determining the right pattern of spread of the LAs [8]. In the developing world accessibility to the US is limited, and hence, use of PNS for such an easy and superficial block increases the utilization and benefits wider population. In this report, we have described the use of PNS for PEC-I block that can be used as a sole analgesia technique for breast implant insertion, pacemaker implantation, port-acath insertion, ICD insertions or removals, and pectoralis muscle flaps. The PEC-I block can be further combined with PNS guided serratus anterior plane (SAP) block [19]to achieve excellent analgesia of the chest wall for surgeries such as breast surgeries, modified radical mastectomy, thoracotomies, LD flaps, and other hemithorax surgeries.
Our Experience After obtaining institutional ethical committee clearance, the authors have used this technique in more than 100 cases and documented the spread of LA using ultrasound following PNS guided injection of the drug and noticed satisfactory deposition and spread in the myofascial plane between the two pectoralis muscles as described in the literature for US-guided PEC-I block. (Fig. 5 and 6) We observed better post-operative pain relief when this block was combined with SAP block.
Limitations The PEC-I block has been described as a safe and superficial block for chest wall procedures, but the concern for pneumothorax remains. The block needs to be done with caution, and conscious attempt is made to remain superficial and lateral as described in the technique. Although with our experience in the number of cases done, we have not encountered any complications yet, larger studies need to be done to establish the safety of the technique compared to other modalities.
Conclusion
As per the literature, the PEC-I block along with PEC-II or SA plane block has a high success rate and minimal incidence of complications and provides a consistent and reliable block for hemithorax analgesia particularly for breast surgeries, wide pectoral dissections, upper chest injuries, and many other procedures such as pacemaker insertions, port-a-cath placements, and intercostal chest drains. In this article, we describe PEC-I block using PNS which is easily available to most anesthetist, unlike US machines which are available only to very few. PNS guided PECI block will increase the scope of this superficial, easy, and reliable block.
References
1. Klein SM, Bergh A, Steele SM. Thoracic paravertebral block for breast surgery. Anesth Analg 2000;90:1402-5.
2. Moon EJ, Kim SB, Chung JY, Song JY, Yi JW. Pectoral nerve block (pecs block) with sedation for breast conserving surgery without general anesthesia. Ann Surg Treat Res 2017;93:166-9.
3. Gartner R, Jensen MB, Nielsen J, Ewertz M, Kroman N, Kehlet H. Prevalence of and factors associated with persistent pain following breast cancer surgery. JAMA 2009;302:1985-92.
4. Lynch EP, Welch KJ, Carabuena JM, Eberlein TJ. Thoracic epidural anesthesia improves outcome after breast surgery. Ann Surg 1995;222:663-9.
5. Blanco R. The “Pecs block”: A novel technique for providing analgesia after breast surgery. Anaesthesia 2011;66:847-8.
6. Blanco R. Bloqueo pectoral (pecs block). Manual de Anestesia Regional y Econoanatomıa Avanzada. Spain: EneEdiciones; 2011. p. 92-5.
7. Blanco R, Fajardo M, Maldonado TP. Ultrasound description of Pecs II
(modified Pecs I): A novel approach to breast surgery. Rev Esp Anestesiol Reanim 2012;59:470-5.
8. Bashandy GM, Abbas DN. Pectoral Nerves I and II blocks in multimodal analgesia for breast cancer surgery: A randomized clinical trial. Reg Anesth Pain Med 2015;40:68-74.
9. Morioka H, Kamiya Y, Yoshida T, Baba H. Pectoral nerve block combined with general anesthesia for breast cancer surgery: A retrospective comparison. J Am Clin Rep 2015;1:1-5.
10. Nair AS, Sahoo RK, Ganapathy M, Mudunuri R. Ultrasound guided blocks for surgeries/procedures involving chest wall (Pecs 1, 2 and serratus plane block). Anaesth Pain Intensive Care 2015;19:348-51.
11. Porzionato A, Macchi V, Stecco C, Loukas M, Tubbs RS, de Caro R. Surgical anatomy of the pectoral nerves and the pectoral musculature. Clin Anat 2012;25:559-75.
12. Gonzales J. PECS versus PVBS for perioperative analgesic management in breast surgery. ASRA News 2016;16:41-4.
13. Naja ZM, El-Rajab M, Al-Tannir MA, Ziade FM, Tayara K, Younes F, et al. Thoracic paravertebral block: Influence of the number of injections. Reg Anesth Pain Med 2006;31:196-201.
14. Moore DC. Intercostal nerve block: Spread of India ink injected to the ribs costal groove. Br J Anaesth 1981;53:325-9.
15. Tobias MD, Ferrante FM. Complications of paravertebral, intercostal, and interpleural nerve blocks. In: Finucane BT, editor. Complications of Regional Anesthesia. Philadelphia, PA: Churchill Livingstone; 1999. p. 7793.
16. Shanti CM, Carlin AM, Tyburski JG. Incidence of pneumothorax from
intercostal nerve block for analgesia in rib fractures. J Trauma 2001;51:536-9.
17. Cheema S, Richardson J, McGurgan P. Factors affecting the spread of bupivacaine in the adult thoracic paravertebral space. Anaesthesia 2003;58:684-7.
18. Cheema SP, Ilsley D, Richardson J, Sabanathan S. A thermographic study of paravertebral analgesia. Anaesthesia1995;50:118-21.
19. Roy R, Singh SK, Agarwal G, Pradhan C. Peripheral nerve stimulator guided serratus anterior plane block: A novel approach to the chest wall block. J Anaesth Crtical Care Case Rep 2017;3:24-6.
| How to Cite this Article: Roy R, Singh S K, Agarwal G, Pradhan C. Peripheral nerve stimulator guided pectoralis (PEC-I) block: A novel approach to the chest wall block. Journal of Anaesthesia and Critical Care Case Reports Jan-April 2018; 4(1):31-34. |