Vol 6 | Issue 1 | January-April 2020 | page: 3-5 | Gaurav Vinod Patil, Chi Ng
Author: Dr. Gaurav Vinod Patil [1], Dr. Chi Ng [2]
[1] Senior Clinical Fellow (MTI)
[2] Consultant, RCoA College tutor
Department of Anaesthetics & Intensive Care, Barnet and Chase Farm Hospitals, Royal Free London NHS Foundation Trust, North Central London, England, UK
Address of Correspondence
Dr. Gaurav Vinod Patil,
Barnet and Chase Farm Hospitals, Royal Free London NHS Foundation Trust, North Central London, England, UK
E-mail: gasmangp87@gmail.com
COVID-19 experience from an Intensive Treatment Unit (ITU) in London
This article will try to provide an insight into the CoViD – 19 situation in Barnet Hospital with regards to management of the hospital, disease pattern, ITU admission criteria & treatment plans, work pattern of doctors, staff safety, & a trainee doctor’s experience. Barnet Hospital is a District General Hospital (DGH) in North London, whereas, Chase Farm Hospital is an elective surgical Hospital in North East London.
Overall management
Barnet Hospital is a DGH with 450 beds which includes 2 wings of ITU consisting of 10 beds & 13 beds respectively. There are more than 100 confirmed cases, and they are increasing. During the emergency period, elective surgeries have been stopped. The only surgeries that are on are emergencies, trauma (directed to another dedicated trauma centre), cancer surgeries, and maternity. The high risk areas are Emergency dept., isolation wards (separate for confirmed cases and suspected cases), ITU, Theatres, & Maternity. These have been reasonably well stocked with Personal Protective Equipment (PPE).
ITU expansion plan
2 extra beds have been setup in ITU North wing. Theatre recovery has been converted to an 8 bedded ITU with anaesthetic machines as ventilators. A ward adjacent to ITU South wing has been converted to an ITU wing with 6 beds with anaesthesia machine ventilators. That has expanded the ITU capacity to 39. If more beds are needed, 3 out of 5 Operation Theatres and Anaesthetic rooms will be converted to 9 beds with anaesthesia machines as ventilators. Anaesthesia machines have been transported from Chase Farm Hospital.
There is also a plan to transfer acute patients, preferably with single organ failure, to other hospitals with less patient volume, and also a new facility (Nightingale Hospital, Excel Centre) with 4000 dedicated beds for CoViD-19 patients.
Diagnosis
Patients are coming in with a combination of any of the following symptoms : Fever, dry cough, sore throat, history of recent travel/contact, shortness of breath, relatively less work of breathing for the degree of hypoxia. Bizarre presentation with GI symptoms have also been reported.
Labs
Typically show lymphopenia, raised CRP, n o r m a l P C T ( i f r a i s e d , c a n h a v e superimposed bacterial infection), bilateral ground glass infiltrates on Chest X–ray. Raised Ferritin, Troponin I (myocarditis) are other markers that are measured, which indicate a poor prognosis.
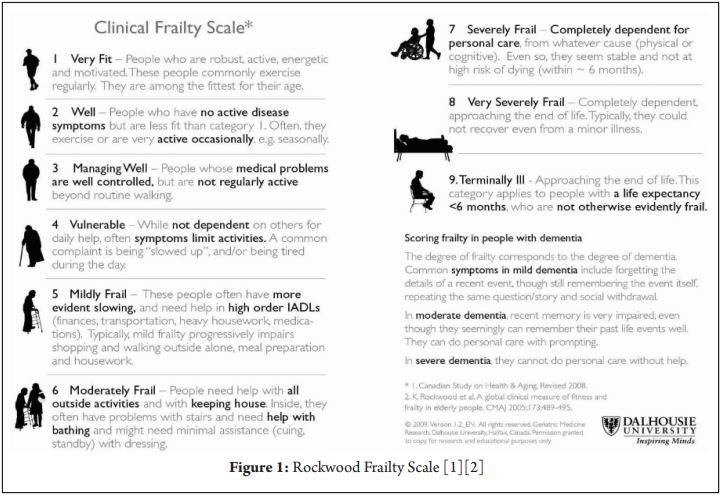
ITU admission criteria
We are generally accepting patients based on those that would most benefit from ICU treatment. The Rockwood Frailty Scale is an example (see Fig 1). More importantly, a documented treatment escalation plan is a must for each patient based on discussions with the patient and family. We have not had to refuse treatment so far in anyone we thought would be appropriate. Indications for escalation would include hypoxia resistant to conventional oxygen therapy, fatigue or organ support.
Treatment in ITU
Arterial line and serial ABGs to monitor PO2, PCO2, pH, any metabolic component.
O2 by venturi mask– generally target SPO2 > 88%.
Gentle to aggressive diuresis with loop and thiazide diuretics may be appropriate in some cases.
Antibiotics are based on clinical, radiological a n d b i o c h e m i c a l m a r k e r s s u c h a s Procalcitonin.
CPAP is considered, albeit cautiously and for a limited period of time.
Optiflow has been used with limited success in a couple of patients but the high aerosolization rate and high oxygen consumption make it difficult.
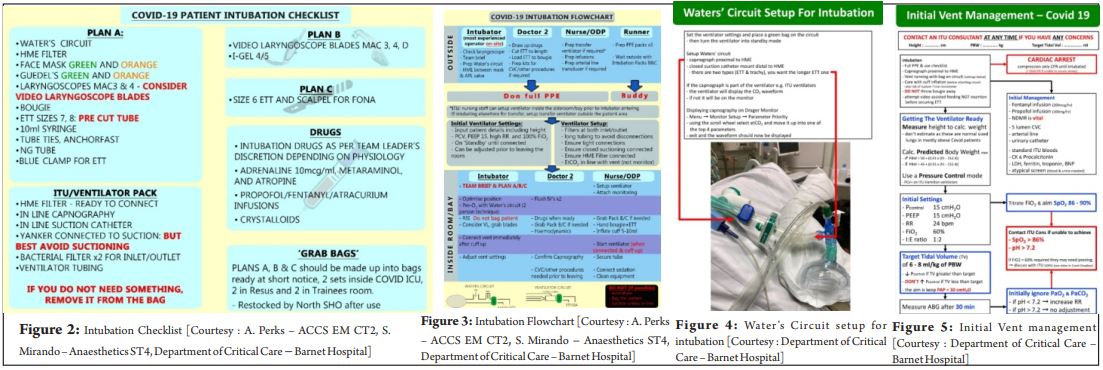
In the majority of patients, intubation and mechanical ventilation is required. PCV or ASV with an initial high PEEP is used and then readjusted based on response.
Patients usually require paralysis for 24 – 48hrs.
Early proning has been advantageous in improving oxygenation but its long term effects are unknown (we have a dedicated proning team consisting of different specialties).
We have noticed a high incidence of renal dysfunction, so fluid balances have been very important. We also have limited capacity for renal replacement therapy on the unit and this has been an issue.
ECMO is a last resort but requires referral to a suitable centre.
Staff & equipment safety
3 HME filters are being used to protect ventilators, one at the patient end, & one on each limb of the vent circuit.
Doctors use full PPE for proven and highly suspected cases for ITU referrals. There are dedicated donning and doffing areas in theatres, ITU, Emergency dept. Also, there are daily simulation drills for staff, in case a confirmed or suspected case came to theatre/maternity for an emergency surgery, C-section.
Aerosol generating procedures (AGP) included intubation, extubation, open suctioning, CPR. For these, full PPE is required.
Full PPE – Cap covering ears/ hood, eye protection glasses/Visor (prefer visor for AGPs), FFP3 mask (mask fit testing to be done preferably), gloves followed by water repellent gown (tie around) followed by another pair of gloves above the gown (taped so that they can come out with the gown), followed by a 3rd pair of gloves; plastic apron over the gown, water resistant (plastic or rubber) clogs.
The 3rd pair of gloves and plastic apron are changed after seeing one patient, and the entire PPE is changed after performing an AGP.
Sickness
Doctors with symptoms have to isolate for 7 days, then join back if they feel better & are afebrile. Sickness cover is put out as a locum shift. There is going to be a provision for testing staff that are experiencing symptoms. The trust has setup a CoVid advice helpline and email which is very helpful to staff with symptoms.
Duty rotations
The department consists of 24 anaesthetic consultants, 6 staff doctors, 12 ITU consultants, and 46 trainees at various levels ranging from junior fellows, core trainees, and specialist trainees.
Trainee shifts are 13hr shifts 0800 – 2100 or 2000 – 0900. There are 6 – 8 trainees on call at a time with 1 resident anaesthetic consultant, 1 anaesthetic consultant on standby, 1 ITU consultant (home after midnight). The rota for a trainee currently is 3 days of work, followed by 3 days off, followed by 3 days standby (can be called in, for atleast 1 shift). If we are standby on a weekend and are called in, we get paid as locum.
Some Dos and Don’ts for healthcare workers on the frontline.
Dos
1) Frequent hand washing for atleast 20 sec with soap and water/alcohol based handrub, both at and off work.
2) Use your foot/leg/shoulder/back to open/push doors etc.. If unavoidable, use your non-dominant hand for it.
3) Change into scrubs as soon as you reach work.
4) Follow a decontamination routine after you reach home. Keep dedicated areas/boxes for contaminated clothes. Shower as soon as you reach home, and then preferably wash your clothes separately, and then wash your hands before you enter clean areas.
5) Maintain distance from vulnerable family members, especially elderly.
6) Use proper PPE at work.
Don’ts
1 ) A v o i d t o u c h i n g y o u r face/eyes/nose/mouth/ears, especially at work. If you have to, think twice if your hands are clean. Wash them first. You are unlikely to use your nondominant hand to touch your face. So use it for pulling door handles.
2) Don’t be careless during and after doffing. Proper Disposal of PPE used by you is your responsibility. Most importantly, don’t let your mask dangle around your neck. Use it, and then throw it immediately after use.
3) Don’t dispose your scrubs on the floor in the changing rooms. Put them in disposal bins/scrub machines.
4) Don’t venture out after work unless absolutely necessary, in accordance with government advice. If it is important, shower at work before.
5) Don’t neglect handwashing.
My personal experience while working during this crisis-
Until February, I was quite naïve about the situation as I was reading the trust emails about the plans, policies & SOPs. I had got my mask fitting done, along with training for donning and doffing the PPE. Reality hit me when I entered the hospital on a night shift in mid-March & saw the COVID warning notices on the doors of one of our ITU wings where I was supposed to work. I realised that it was time to actually don the PPE, work in it, and then doff properly; and I needed to do it multiple times during every shift in the coming few weeks, if not months. The fear of contracting the infection from one of the patients was & is always there at the back of my mind, but, I think I just get on with it like the rest of my colleagues, because that is what we doctors and nurses are taught – The patient always comes first.
The rota has changed as mentioned above. The working hours are more or less similar,
but the shifts are much busier than usual. Teamwork is the key now, more than ever, and I will proudly say that we have coped well so far. Any patient admitted to ITU needing intubation is handled by teams of 3 doctors, either 1 consultant and 2 trainees, or 3 trainees (atleast 2 senior trainees). The drill is, preferably, to site an arterial line, followed by intubation & NG tube insertion, followed by CVC insertion. Performing procedures in PPE is an altogether different ball game, especially with 4 gloves and 2 gowns on. Also, we are proning more patients more frequently than ever which is labour intensive, and that’s where teamwork comes in handy, especially with help from surgical and orthopedic colleagues.
As we expanded to new areas (ward & recovery), new challenges have come up with managing COVID pneumonia patients with anaesthetic machine ventilators. We have to check and replace the sodalime canisters and HME filters frequently. Also, we have to look for water accumulation in the circuit and empty it from time to time. Also, there is a learning curve for ITU nurses for getting used to the anaesthetic machine ventilators, which means that we as doctors have to be more vigilant.
Another challenge that we all face, is communicating with the next of kin of the patients. That usually happens over the phone, as they are in self isolation themselves most of the time, and were not allowed to visit them in the hospital or ITU initially, although there is a provision for that now. It is difficult to communicate with them, especially if the patient’s condition is deteriorating. Most of the times, I could give the patients the opportunity to talk to their family before taking them to ITU, but not always, as some deteriorated very quickly. This entire situation takes a toll on our mental health as well. The trust has a helpline in place for staff having mental health issues, even before the CoVid pandemic started.
I also had the experience of transferring 3 of these patients to other hospitals. I had to transfer them alone along with the ambulance crew paramedics of London Ambulance Services as we were short staffed in the nursing department. Transferring them in PPE had its own challenges, but the ambulance crews were extremely helpful.
There have been significant changes in my work-life balance. At home, considerable amount of time is spent reading and watching news about the pandemic, especially since my family is in India. I am communicating with them frequently to allay their anxiety about the rapidly developing situation in the UK. I also have set a decontamination routine before entering my flat. My wife is at home as her part time job had stopped due to the lockdown. I have isolated myself in a separate room, as I am a potential risk to her. We also have to find new ways of entertaining ourselves, while also maintaining social distancing.
In spite of the precautions at home and work, I experienced dry cough and bodyache in the 2nd week of April, & that is when I decided to call-in sick. I was asked to self-isolate for 7 days. My wife was asked to do the same for 14 days, but her symptoms started 2 days later. I got tested, & 24 hrs later I came to know that I had tested positive. That was, ironically, the exact same day when I had fever, which went on for 2 more days. On one hand, we both were being strong and were treating it like a flu, but deep down we were scared, because of all the news from around the world, & I was also feeling guilty, because I had probably given it to my wife. Her symptoms got worse after mine, which also included some degree of breathlessness.
We supported each other well during this time of isolation. A friend was really helpful & dropped off some groceries. We decided not to tell our families, as they would get stressed & feel helpless. After the 5th day of symptoms, my temperature was normal & I started feeling better. My wife experienced the same thing, but she had lost her taste & smell sensation. We both have recovered now and I have resumed work.
There is a bright side to this that we are connecting with friends and family, more often than we usually would. Also, there has been a lot of appreciation from the general public and corporate brands for healthcare professionals in the form of applauses, videos, discounts, free food deliveries to hospitals and homes, and also some free goodies. All this appreciation encourages us to march further in the fight against this deadly virus.
Conclusion
This pandemic has given me a ‘once-in-a-lifetime’ experience of a crisis situation and continues to test; not only my professional knowledge, application & efficiency as a doctor; but also; my character, strength, resilience, & courage as a human being. I am fairly confident that we all will emerge out of this situation, victorious! Take care. Stay safe.
References
1. Canadian Study on Health & Aging, Revised 2008.
2. K. Rockwood et al. A global clinical measure of fitness and frailty in elderly people. CMAJ 2005; 173: 489-495.
| How to Cite this Article: Patil GV, Ng C | COVID 19 experience from an Intensive Treatment Unit (ITU) in London | Journal of Anaesthesia and Critical Care Case Reports | Jan-April 2020; 6(1): 3-5. |
(Full Text HTML) (Download PDF)