Vol 5 | Issue 3 | Sep-Dec 2019 | page: 16-17 | Shilpi Sethi, Prashant Gupta
Authors: Shilpi Sethi [1], Prashant Gupta [1]
Address of Correspondence
1 Department of anaesthesia, Sitapur Eye Hospital and Regional Institute Of Ophthalmology, Sitapur, Uttarpradesh, India.
Dr. Shilpi Sethi,
Sitapur Eye Hospital and Regional Institute Of Ophthalmology, Sitapur, Uttarpradesh, India.
E-mail: shilpisethi77@gmail.com
Abstract
Introduction: Xeroderma Pigmentosum (XP) although a rare disease, characterized by deficiency in Nucleotide Excision Repair (NER) mechanism, making one susceptible to UV induced hypersensitivity of skin at an early age. Thereby children present with neoplasm of skin, mucous membrane and ocular surfaces often requiring surgeries.
Case Presentation: We report a 10 year old female patient with Xeroderma pigmentosum who presented with scleral nodule requiring excision under general anaesthesia. Inhalational anaesthetics, paracetamol and opioids may cause genotoxic side effects in patients with defects in Nucleotide excision repair. Airway is often compromised due to buccal cavity scarring. We adopted a Total intravenous anaesthesia technique (TIVA) technique using propofol, dexmedetomidine, I gel and medial canthal peribulbar block for analgesia.
Conclusion: The aim of this case report is to highlight the anaesthetic implications like anticipation of difficult venous access, meticulous airway evaluation and judicious use of total intravenous anaesthesia. The psychosocial aspect of Xeroderma pigmentosum should also be dealt with in educating the parents in avoiding sun exposure, using UV creams and need for repeated surgeries.
Keywords: Xeroderma Pigmentosum, Nucleotide Excision Repair, TIVA.
Introduction
Xeroderma Pigmentosum (XP) is a rare autosomal recessive disease with failure to repair UV induced DNA lesions due to defect in Nucleotide Excision Repair (NER) mechanism. This results in premature development of skin neoplasms. Face and lips are particularly involved. Approximately 80% of Xeroderma pigmentosum patients have ocular involvement in the form of keratitis, cataract and eye tumours [1]. 20% have progressive neurological complications [2].
Case Report
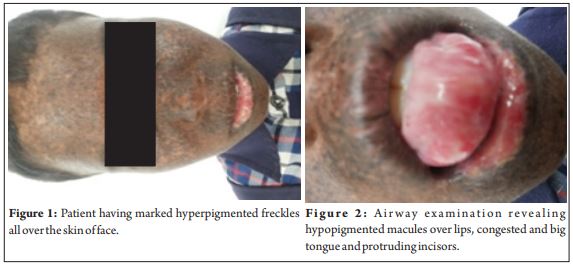
Ten year old female patient weighing 23kg with the clinical diagnosis of XP presented with painful scleral nodule in the left eye requiring excision under generalanaesthesia . She had marked hyperpigmented freckles all over the skin of face (Fig 1), trunk and extremities. She also complained of photophobia and dry eyes. There was no cognitive dysfunction and neurological examination was normal. Airway examination revealed hypopigmented macules over lips, congested and big tongue and protruding incisors (Fig 2). Mouth opening, and neck movements were normal. Mallampatti grade was 2. General examination was unremarkable and all investigations were within normal limits. Intravenous cannulation was done after application of EMLA cream. After premedication with injection atropine 0.02 mg/kg , preoxygenation, injection dexmedetomidine 1mcg/kg was given over 10 minutes. Monitoring included NIBP, SPO2, ECG, and ETCO2. Patient was induced with injection propofol 2mg/kg and injection ketamine 0.25 mg/kg was and IGel size 2 placed in a single attempt. Controlled ventilation was achieved using injection atracurium 0.3 mg/kg and dexmedetomidine infusion given at the rate of 0.2mcg/kg/hr. Inhalational anaesthetics were completely avoided and 50% mixture of oxygen and nitrous oxide was used for ventilation. A single medial canthal peribulbar block with 3ml of 0.5% bupivacaine given for analgesia. Surgery lasted 45 minutes, dexmedetomidine stopped, neuromuscular blockade reversed, and IGel removed. Haemodynamics was maintained within normal limits. No bradycardia observed in spite of using dexmedetomidine a s we routinely premedicate our patients with atropine in order to prevent oculocardiac reflex. Intraoperative and postoperative period was uneventful.
Discussion
XP is notorious for extreme sun sensitivity causing facial pigmentation by two years of age and skin cancers by eight years [3]. Although the prevalence of XP is rare, it is not uncommon to sight children presenting with premalignant lesions and neoplasms of skin and eye mandating surgery. Literature is replete with plethora of information on the anaesthetic management, yet there is no clear cut consensus. First and foremost is difficult venous access due to dark mottled and freckled skin impairing visualisation. Then comes nodular facial lesions that make mask ventilation challenging. Oral cavity often features marked scarring, actinic cheilitis, big tongue and telangiectasias. Bharti et al [4] reported the use of McCoy levering laryngoscope for successful intubation in eight year child with XP for basal cell carcinoma excision from scalp with Mall ampatti grade 3. It ha s been contemplated that paracetamol and volatile anaesthetics are genotoxic in patients with defects in NER. Comment assays by Karabiyik et al [5] revealed lymphocytic DNA damage at 1 hr and 2 hrs with 1 to 1.5% halothane, isoflurane and sevoflurane. Moreover, Miyazaki [6] did report a further aggravation in neurological symptoms though short lived in postoperative period after using sevoflurane in a patient with XP. Fjouji et al [7] expressed similar concerns regarding use of volatile agents. Further experiments and research is warranted to completely refute the use of sevoflurane which is invaluabl e in pa ediatric anaesthesia. There has been renewed interest in TIVA and dexmedetomidine has been used as a valuable adjunct in a case series of XP patients by Shreshtha et al [8] Oliviera et al [9] recommended minimal usage of muscle relaxants that too under monitoring. Therefore, we utilized IGel and chose TIVA technique using propofol and dexmedetomidine infusion and employing peribulbar block for analgesia.
Conclusion
Meticulous airway evaluation and judicious use of TIVA cannot be overemphasized. BIS guided TIV [10] and neuromuscular monitoring is certainly advocated for well equipped centre. As anaesthesia providers, it is imperative that the psychosocial aspect of the disease burden should also be taken into consideration. Avoiding sun exposure, using UV blocking creams, and need for repeated surgeries need to be explained to the family.
Clinical Message
It is not unusua l for a paediatric anaesthesiologist catering to whole array of ophthalmic, plastic and oncology surgeries to encounter this entity and knowledge, preparedness and skills to handle such cases is certainly required.
References
1. Lopes-Cardoso C, Paes da Silva Ramos Fernandes LM, Ferreira-Rocha J, Teixeira- Soares C, Antônio-Barreto J, Humberto-Damante J. Xeroderma Pigmentosum – A case report with oral implications. J Clin Exp Dent. 2012;4(4):e248-51.
2. Feller L, Wood NH, MotswalediMH,Khammisa RA, MeyerM, et al. Xeroderma pigmentosum: A case report and review of the literature. J PrevMed Hyg 2010;51(2):87-91.
3. Mulimani SM, Talikoti DG. A child with xeroderma pigmentosum for excision of basal cell carcinoma. Saudi J Anaesth. 2013;7(4):467-9.
4. Bharti AK, Kumar N, Kumar AAM, Gupta BK, Suman S. Anaesthetic Management of Siblings having Xeroderma Pigmentosum: A Rare Presentation. J AnesthCrit Care Open Access 2016;4(2):00129.
5. Karabyk L,Sardas S, Polat U, Kocabas NA, Karakaya AE. Comparison of genotoxicity of sevoflurane and isoflurane in human lymphocytes studied in vitro using the comet assay. Mutation Res/ Genetic Toxicol Environ Mutagen 2001;492:99-107.
6. Miyazaki, Ryohei& Nagata, Taro & Kai, Tetsuya & Takahashi, Shosuke. Anesthesia for a patient with xeroderma pigmentosum. Masui. The Japanese journal of anesthesiology. 2007;56:439-41.
7. Fjouji S, Bensghir M, Yafat B, Bouhabba N, Boutayeb E,Azendour H, Kamili ND. Postoperative neurological aggravation after anesthesia with sevoflurane in a patient with xeroderma pigmentosum: a case report. Journal of medical case reports 2013;7:73.
8. ShreshthaGS, Shah RP, Amatya AG, Shreshtha N. Anaesthetic management of patients with Xeroderma Pigmentosum. A series of three cases. Nepal Med Coll J 2011;13(3):231-232.
9. Oliveira CR, Elias L, Barros AC,Conceicao DB. Anesthesia in patient with Xeroderma Pigmentosum. Case Report Rev Bras Anestesiol. 2003 Feb;53(1):46-51.
10. Shah SB, Hariharan U, Naithani BK, Bhargava AK. Clinical Pearls in Anesthesia for Xeroderma Pigmentosum: A Case Report. The Open Anesthesiology Journal. 2015;9:36-38.
| How to Cite this Article:Sethi S, Gupta P | Anaesthetic Dilemma in Paediatric Patients with Xeroderma Pigmentosum: A Case Report | Journal of Anaesthesia and Critical Care Case Reports | Sep – Dec 2019; 5(3): 16-17 |
(Full Text HTML) (Download PDF)
.