Vol 3 | Issue 1 | Jan-Apr 2017 | page: 20-23 | Deepak P Madankar, Neelesh K Mathankar.
Authors: Deepak P Madankar [1], Neelesh K Mathankar [1]
[1] Department of Anaesthesiology and Pain Medicine, Meditrina Institute of Medical Sciences, Nagpur, Maharashtra, India.
Address of Correspondence
Dr. Deepak P Madankar,
Department of Anaesthesiology and Pain Medicine, Meditrina Institute of Medical Sciences,
Nagpur, Maharashtra, India. Phone: +91-9850332882.
E-mail: deepakmadankar30@gmail.com
Abstract
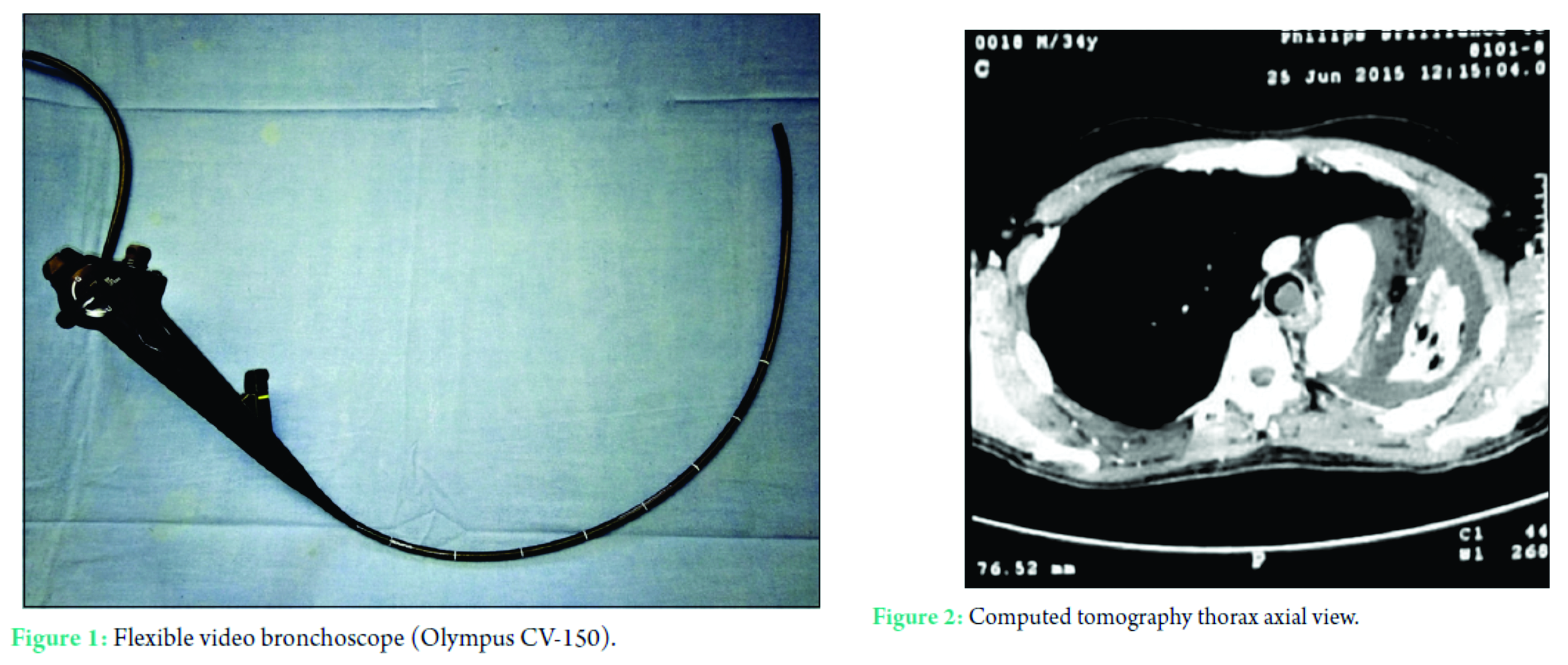
Background: Lung separation in the presence of significant tracheal lumen narrowing due to intratracheal-carinal mass, possess unique challenge to the anesthesiologist. In conventional flexible video bronchoscope (FVB) (Fig. 1)-guided double-lumen tube (DLT) insertion, the field of vision is distal to the tube, which does not completely mitigate the risk of traumatic bleeding and dislodgement of the mass.
Case Presentation: A 35-year-old male with metastatic dermatofibrosarcoma protuberans (DFSP) with complete left lung involvement and intratracheal-carinal extension of the tumor was scheduled for left pneumonectomy. Left lung parenchymal lesion was extending intraluminally along the left main bronchus up to the carina and tracheal lumen causing significant obstruction at carina.
Conclusion: In this case report, we present first successful use of a novel FVB-DLT side-by-side technique, where one anesthesiologist holds the FVB to keep the mass in focus and second anesthesiologist maneuvers the DLT to bypass the mass through the narrowed tracheal lumen under FVB vision.
Keywords: Flexible video bronchoscope, double-lumen tube, intratracheal-carinal mass, lung separation.
Introduction
Resection of intratracheal mass always poses a challenge to anesthesiologists. Since airway is shared by both surgeon and anesthesiologist, it is essential to maintain ventilation, while allowing free surgical access at the same time [1]. It becomes particularly more challenging if the tumor involves entire one lung because salvage of healthy lung from spoiling becomes an additional concern. Various methods for airway management during anesthesia for endotracheal mass have been described [2, 3, 4, 5, 6]. We report a case of metastatic dermatofibrosarcoma protuberans (DFSP) with complete left lung involvement and intratracheal-carinal extension of the tumor intubated successfully with right-sided double-lumen tube (DLT) guided by fiberoptic bronchoscope vision.
Case Report
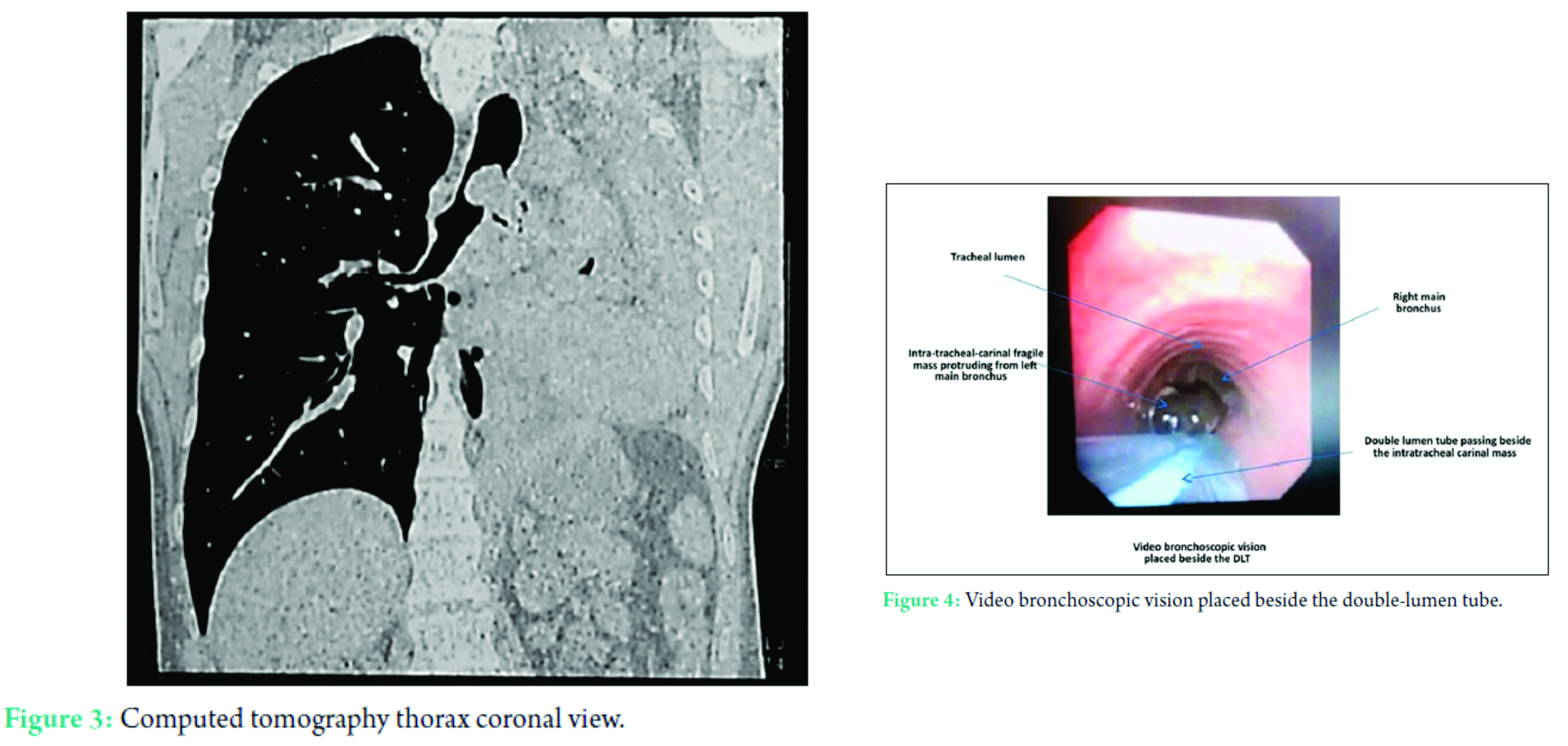
A 35-year-old male patient, who is a known case of anterior abdominal wall DFSP with left lung metastases and complete parenchymal collapse, was scheduled for left pneumonectomy. Computed tomography (CT) chest revealed large left lung parenchymal lesion extending intraluminally along the left main bronchus up to the carina and tracheal lumen causing significant obstruction at carina (Figs. 2 and 3). Diagnostic flexible video bronchoscopy showed complete luminal obstruction of left main bronchus with soft tissue mass protruding into carina and tracheal lumen. Pre-operative assessment revealed absent breath sounds on left side on chest auscultation and oxygen saturation of 97% on room air. Other relevant clinical examination and blood investigations were within normal limits. CT pulmonary angiography showed complete obstruction of lumen of left pulmonary artery by the hilar soft tissue. Two-dimensional (2D) echocardiogram revealed normal left ventricular function and no pulmonary hypertension or right ventricular strain. After an informed consent patient was posted for surgery in ASA Grade III. In the OR, standard monitoring was applied, and thoracic epidural catheter was inserted under local anesthesia at D7-D8 level for post-operative pain relief. An awake flexible video bronchoscope (FVB)-guided, 32F size, right-sided DLT placement was planned in view of carinal luminal narrowing. The patient was pre-medicated with glycopyrrolate 0.2 mg, fentanyl 1 mcg/kg, and midazolam 1 mg; and a structured local anesthesia regimen was applied to achieve upper airway anesthesia.
FVB-DLT side-by-side technique was applied for intubation, where one anesthesiologist holds the FVB to keep the mass in focus and second anesthesiologist maneuvers the DLT. Initially, the FVB was inserted orally and passed two centimeters below the vocal cords and FVB view is stabilized by one anesthesiologist. Then, the second anesthesiologist performed direct laryngoscopy and passed a 32 F right-sided DLT through vocal cords. The DLT is maneuvered to pass through the narrowed tracheal carinal lumen beside the lesion under direct vision without touching or traumatizing the mass (Fig. 4).
The correct position of DLT including proper right upper lobe ventilation was confirmed by FVB and auscultation. Post-intubation examination of mass revealed no trauma or bleeding from it. General anesthesia was then administered with 120 mg propofol and 6 mg of vecuronium and maintained with oxygen-nitrous oxide sevoflurane combination. The patient was ventilated with tidal volume of 300-350 ml with peak airway pressure of 18-22 mmHg to maintain end tidal CO2 of 35-40 mmHg. After completion of surgery, FVB examination of left bronchial suture line revealed no leaks or bleeding. The patient was extubated after adequate neuromuscular blockade reversal and sensorium. Post-operative pain relief was ensured by thoracic epidural analgesia. His recovery was uneventful and he was discharged from the surgical ward on 7th day.
Fig: Novel techinique of FVB guided DLT insertion in a case of metastatic intratracheal carinal mass
Discussion
DFSP is a relatively unusual fibrohistiocytic tumor that is classified as an intermediate-grade malignancy. DFSP is characterized by infiltrative growth and a high propensity for local recurrence after surgical excision. Although metastasis is rare, lung metastasis is the most common, while the lymph node metastasis is exceedingly rare [7]. Although mostly seen in middle age, a few cases have been described in infants and children. In our case, the patient is middle aged, which is the common age group, and has lung metastasis. Ventilation and maintaining oxygenation are specific challenges during tracheobronchial resection surgery. However, in this case, the challenge was to isolate the lung to prevent spillage. Isolation of lung to prevent spillage from hemorrhage or infection is an
absolute indication for one lung ventilation [8]. Double-lumen endotracheal tube placement is the most common way of separating the two lungs [9]. Right DLT is indicated when the surgery involves left main bronchus. Placement of DLT by sliding over the FVB is a documented technique but has its own limitation that the field of vision is always distal to the DLT. Hence, this technique does not completely mitigate the risk of accidental trauma and dislodgement of the mass while sliding the tube. Hence, we implied FVB-DLT side-by side technique, where DLT was maneuvered under direct FVB vision minimizing the risk of accidental trauma or dislodgement of mass. There are two considerations related to selecting size of a DLT. The main body of the tube must pass through the glottis and advance down the trachea without causing trauma, and the bronchial component must be able to enter the intended bronchus [10]. We selected smaller 32 F DLT because there was a significant tracheal lumen narrowing due to tumor. It was not possible to pass the regular size of 39-41 F DLT without injury to the mass. The bronchial cuff of this smaller DLT was inflated with larger volumes of air for proper lung isolation. Although the smaller DLT offers more resistance to airflow during one-lung ventilation, the airway pressures were well maintained within normal limits in our patient. After induction of anesthesia, loss of smooth muscle tone decreases the diameter of the patent lumen [11]. Thus, intubating the trachea after induction of anesthesia in such patients is more dangerous because of increased risk of bleeding. For the same reason, we preferred awake intubation in our patient. In literature search, we could find only one case report where authors have used similar technique unsuccessfully. Liou et al. explained that the tumor in their case was just 2 cm below the vocal cords so it was difficult to stabilize the bronchoscopic vision [11]. However, in our case, the mass was in lower half of the trachea, so not only we could stabilize the FVB vision but also maneuvered the DLT easily.
Conclusion
In rare clinical scenario, where lung separation is indicated in the presence of significant tracheal lumen narrowing due to intratracheal-carinal mass, this novel FOB-DLT side-by-side technique can be used successfully. The utilization of 2D movement advantage for intratracheal advancement of DLT bypassing the mass in an effective manner makes the technique more attractive.
References
1. Pinsonneault C, Fortier J, Donati F. Tracheal resection and reconstruction. Can J Anaesth 1999;46:439-55.
2. Lin CM, Li JY, Hsu JC, Yang CY. Combined conventional and jet ventilation in airway management in tracheal tumor. Chang Gung Med J 2001;24:455-9.
3. Bouaggad A, Bennani F, Al Harrar R, Bouderka MA, Harti A. Anesthesia for a patient with tracheal tumor using laryngeal mask airway. Anesth Analg 2006;103:258-9.
4. Divatia JV, Sareen R, Upadhye SM, Sharma KS, Shelgaonkar JR. Anaesthetic management of tracheal surgery using the laryngeal mask airway. Anaesth Intensive Care 1994;22:69-73.
5. Ng YT, Lau WM, Yu CC, Hsieh JR, Chung PC. Anesthetic management of a parturient undergoing cesarean section with a tracheal tumor and hemoptysis. Chang Gung Med J 2003;26:70-5.
6. Dabbagh A, Mobasseri N, Elyasi H, Gharaei B, Fathololumi M, Ghasemi M, et al. A rapidly enlarging neck mass: The role of the sitting position in fiberoptic bronchoscopy for difficult intubation. Anesth Analg 2008;107:1627-9.
7. Rosai J. Ackermans Surgical Pathology. St. Louis, MO, USA: Mosby; 2004. p. 184, 185, 2256.
8. Kiyota Y, Hartigan PM, Topulos GP. Lung Isolation techniques. In: Aglio LS, Lekowski RW, Urman RD, editors.
Essential Clinical Anesthesia Review: Keywords, Question and Answers for the Boards. Cambridge: Cambridge
University Press; 2015. p. 279-81.
9. Campos JH. Current techniques for perioperative lung isolation in adults. Anesthesiology 2002;97:1295-301.
10. Brodsky JB, Macario A, Mark JB. Tracheal diameter predicts double-lumen tube size: A method for selecting left doublelumen tubes. Anesth Analg 1996;82:861-4.
11. Liou JY, Chow LH, Chan KH, Tsou MY. Successful anesthetic management of a patient with thyroid carcinoma
invading the trachea with tracheal obstruction, scheduled for total thyroidectomy. J Chin Med Assoc 2014;77:496-9.
| How to Cite this Article: Madankar DP, Mathankar NK. A novel technique for flexible video bronchoscope-guided double-lumen tube insertion in a case of metastatic dermatofibrosarcoma protuberans with intratrachealcarinal mass. Journal of Anaesthesia and Critical Care Case Reports May-Aug 2017;3(3):20-23. |