Vol 9 | Issue 2 | May-August 2023 | Page: 14-15 | Manjusha Sawale, Vinit Bedekar, Anshumala Shukla (Kulkarni)
DOI: https://doi.org/10.13107/jaccr.2023.v09i02.219
Author: Manjusha Sawale [1], Vinit Bedekar [1], Anshumala Shukla (Kulkarni) [1]
[1] Department of Anaesthesiology, Kokilaben Dhirubhai Ambani Hospital, Mumbai, Maharashtra, India.
Address of Correspondence
Dr. Manjusha Sawale
Department of Anaesthesiology, Kokilaben Dhirubhai Ambani Hospital, Mumbai, Maharashtra, India.
E-mail: manjushasawale@gmail.com
Abstract
Interstitial lung disease (ILD) and scleroderma are diseases which are very challenging to anaesthesiologists from the perspective of general anaesthesia1. The patients undergoing laparoscopic surgeries are ever increasing due to its very obvious positives like lesser post operative pain and shorter length of hospital stay along with faster recovery. General anaesthesia forms the mainstay in laparoscopic procedures. Special situations like interstitial lung disease are considered high risk for postoperative pulmonary complications and morbidity,2,3,4. Modification of surgical and anaesthetic techniques forms the mainstay for successful management of such patients for a better outcome and patient safety especially in decompensated disease or tough to treat pathologies. Here, we describe a tailored vNOTES hysterectomy for a patient with interstitial lung disease with bilateral crepitations, scleroderma, hypertension and diabetes successfully managed under regional anaesthesia (combined spinal and epidural anaesthesia).
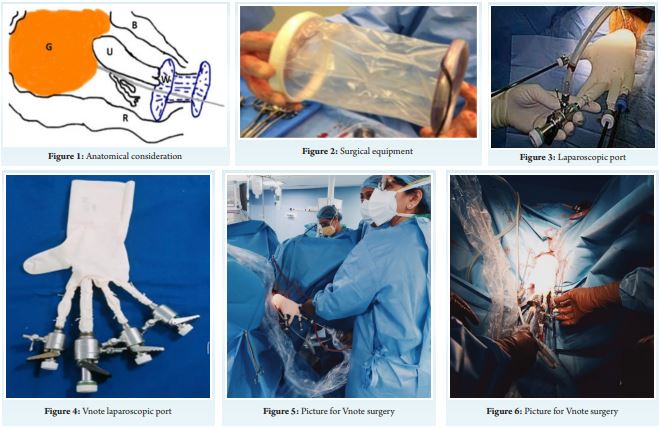
Our patient, a 47 year old, female, weighing 79 kg, a known case of scleroderma, interstitial lung disease (ILD) with history of frequent exacerbations, hypertension, diabetes mellitus and Reynaud’s disease. She had a surgery for renal calculus 6 years ago when there were postoperative lung complications and was then diagnosed with ILD and scleroderma. The patient had bilateral crepitations more on the right side with room air oxygen saturation of 98%, the opinion of both rheumatologist and pulmonologist was taken who suggested regional anaesthesia. After a thorough discussion with the surgeon it was decided that the procedure will be done under regional anaesthesia (combined spinal epidural block) with a modified laparoscopic approach (vNOTES) whereby the ports are placed through the vagina and the CO2 insufflation can be achieved with lower pressures. The patient was optimized preoperatively, high risk consent was taken and a postoperative ICU back up was made available. Once in the OR, standard ASA monitors were attached which included ECG, NIBP, SpO2, ETCO2. A wide bore IV was secured. 500 ML NS iv was used as preloading. With the patient in sitting position, under all aseptic precautions, L1-L2 epidural space was accessed with a midline approach with loss of resistance to air technique, epidural catheter was cited and fixed at 12 cm to skin. The L1-L2 subarachnoid space was accessed using a paramedian approach with a 25G QB needle and after confirming clear and free CSF flow, 3.5 ml of 0.5% bupivacaine hyperbaric with 15 mcg fentanyl was injected. The spinal level was assessed to be at T6. After positioning the patient supine, inj, glycopyrrolate 0.2 mg IV, inj. Midazolam 1 mg iv was given. Inj. Dexmedetomidine @ 0.5 mcg/ kg/ min was started intravenously. The surgery lasted for 2 hours. Patient remained comfortable and hemodynamically stable throughout. Post operatively an epidural infusion of 0.1% ropivacaine was started at 7 ml/ hour. VAS scores remained less than 2 along with multimodal analgesia consisting of inj. Paracetamol 1gm 8th hourly and tramadol 50 mg iv on sos basis. vNOTES is a surgical technique, but a combination of two existing techniques namely the vaginal hysterectomy and the laparoscopic hysterectomy5.
Medically optimizing treatable comorbidities should be a priority in preoperative assessment 2,3. Regional or neuraxial anaesthesia should be considered an optimal technique for the avoidance of general anaesthesia related complications when indicated as followed in our case.1-4
A well placed epidural catheter not only provides excellent analgesia but also helps in improving the post-operative pulmonary function along with the incentive spirometry. Avoidance of general anaesthesia and endotracheal intubation along with a good postoperative analgesia decreases the complication rate in this fragile subgroup of patients.
References
[1] Ryerson CJ, Collard HR. Update on the diagnosis and classification of ILD. Curr Opin Pulm Med. 2013;19(5):453–459. doi:10.1097/MCP.0b013e328363f48d
[2] Ley B, Collard HR, King TE Jr. Clinical course and prediction of survival in idiopathic pulmonary fibrosis. Am J Respir Crit Care Med. 2011;183(4):431–440. doi:10.1164/rccm.201006-0894CI
[3] Carr ZJ, Yan L, Chavez-Duarte J, Zafar J, Oprea A. Perioperative Management of Patients with Idiopathic Pulmonary Fibrosis Undergoing Noncardiac Surgery: A Narrative Review. Int J Gen Med. 2022 Feb 23;15:2087-2100. doi: 10.2147/IJGM.S266217. PMID: 35237071; PMCID: PMC8882471.
[4] Choi SM, Lee J, Park YS, Cho YJ, Lee CH, Lee SM, Yoon HI, Yim JJ, Lee JH, Yoo CG, Lee CT, Kim YW, Park JS. Postoperative pulmonary complications after surgery in patients with interstitial lung disease. Respiration. 2014;87(4):287-93. doi: 10.1159/000357046. Epub 2014 Feb 21. PMID: 24577160.
[5] Wang, X., Li, J., Hua, K. et al. Transvaginal natural orifice transluminal endoscopic surgery (vNOTES) hysterectomy for uterus weighing ≥1 kg. BMC Surg 20, 234 (2020). https://doi.org/10.1186/s12893-020-00897-3
4).
| How to Cite this Article: Sawale M, Bedekar V, Kulkarni A VNOTES Hysterectomy | Under Regional Anaesthesia- A Patient Centric Approach | Journal of Anaesthesia and Critical Care Case Reports | May-August 2023; 9(2): 14-15 | https://doi.org/10.13107/jaccr.2023.v09i02.219 |