Vol 1 | Issue 1 | May – August 2015 | page:21-23 | Raghu S Thota[1].
Author: Raghu S Thota[1], Pooja Baliga[1].
[1] Department of Anesthesia, Dr Panjabrao Deshmukh Memorial Medical College., Maharashtra, India
Address of Correspondence
Dr. Raghu S Thota
Associate Professor, Tata Memorial Centre, Country India.
Email: ragstho24@rediffmail.com
Abstract
Introduction: Bag-mask ventilation (BMV) in edentulous patients or those having their dentures removed is difficult and a challenge to the anaesthesiologist. We have discussed a technique of BMV, by pulling the sunken cheeks upwards with either index or middle finger to form an airtight seal around the mask as well to form an adequate external mask fit. Our manoeuvre improves the BMV effectively with no harm to the patient. It’s a very simple technique and should be used widely to assist ventilation . No special equipment is needed for the technique and by implementing a very minor alteration by pulling the sunken cheek tremendous improvement in BMV can be achieved.
Keywords: Bag mask ventilation, edentulous, cheek
Introduction
Bag Mask Ventilation (BMV) is an important aspect of airway management during anaesthesia[1, 2] as well during emergency airway situations[3, 4]. Bag-mask ventilation (BMV) in edentulous patients or those having their dentures removed is difficult , prevalence of edentulism is high among individuals over 65 years (60%) and due to the problem of proper covering of mask in patients with hollow cheeks (caused by edentulism) BMV has turned into a great challenge in these patients[5, 6, 7]. Routinely in most centres, their dentures are removed prior to being transferred to the operating room. Every anaesthetist faces this problem in edentulous patients and it is one of the predictors of difficult mask ventilation[8]. To overcome this problem various techniques have been used, which include use of smaller face mask, slipping of randell baker saucek mask inside the mouth, use of specially designed anatomical mask, use of oral airway or nasal mask and leaving well fitting denture in place during ventilation[9]. Retaining the denture helps to maintain the shape of facial soft tissues and improve the mask seal[10]. We would like to share our experience by use of an alternate technique to improve bag mask ventilation. This does not require any special equipment. Moreover, it can be used with any anatomical face mask.
Case Series
A 67 years old male patient presented to our institute with pain in abdomen and diagnosed to have moderately differentiated adenocarcinoma of sigmoid colon. He was posted for anterior resection of rectum. He has a past history of hypertension since 8 years on Tab. Amlodepin 5mg OD and verapamil 120mg Sustained released, and type 2 diabetes mellitus on voglibose 0.2mg OD. Physical examination was unremarkable. Preoperative investigations were within normal limits. Patient weighed 63 kgs, 165 cm tall (body mass index 23.14 kg/m2) with a mouth opening of 4.5 cm, edentulous with removable complete artificial denture (fig. 1a), Mallampati grade 1, and jaw slide +1. Written permission & consent to publish in a scientific journal and for photography was taken. In the operating room standard monitors were placed and 1mg IV midazolam along with 75mcg fentanyl injected. After preoxygenation, standard induction included 1–2 mg/kg propofol injected intravenously over 60 s. After loss of consciousness and cough reflex, bag mask ventilation attempted with the routine neck extension and jaw thrust technique with two hands (fig. 1b). There was no chest expansion and no end tidal carbon dioxide reading recorded (fig. 1c). We used our technique to improve bag mask ventilation, where the sunken cheeks are pulled up with either index or middle fingers of both hands to form an airtight seal around the mask and an adequate external mask fit (fig. 1d), which improved bag mask ventilation (fig. 1e). Patient was intubated with 8 Fr cuffed oro tracheal tube (Portex). The remaining intraoperative and post operative period were uneventful.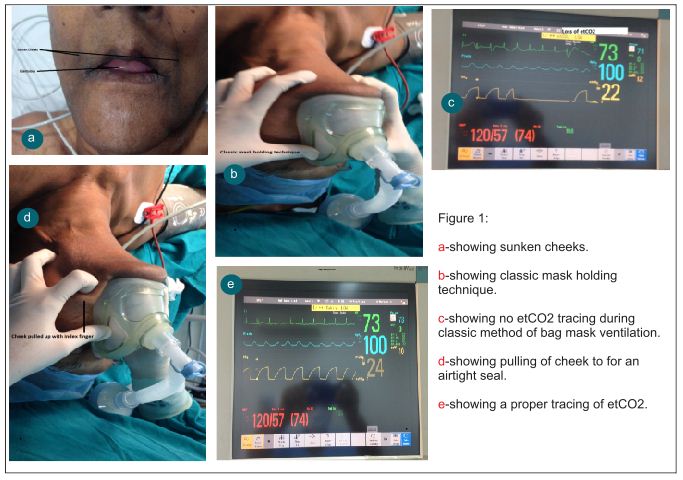
Discussion
Bag mask ventilation (BMV) is a life saving method of controlling airway even in patients with difficult intubation. Weiss and Lutes showed that endotracheal intubation in traumatic patients do not increase the survival rate compared to BMV[11]. During general anaesthesia, reduced muscle tone of oropharynx leads to collapse of tongue, soft palate and epiglottis contributing to airway obstruction as a factor of difficult BMV in anaesthetized patients. Edentulous patients are at increased risk of the obstruction and difficult BMV comparing to patients with teeth[12, 13]. Furthermore, these patients have relatively big tongues due to jaw bones cavity and collapse of the tongue in edentulous patients’ mouth[14]. Mask ventilation is often not effective and, in some cases, almost impossible in edentulous patients because of the lack of facial support. This lack of support leads to an inadequate external mask fit and significant air leaks. Langeron et al[15] suggested not to remove dentures before induction of anesthesia to maintain a proper facial support. However, this may be a dangerous approach because the dentures may be swallowed or aspirated. Nasal positive pressure may be used in edentulous patients because the mask contact is only on the maxillary plane[16]. Another approach consists of placing the caudal end of the mask between the inferior lip and the alveolar ridge[17, 18]. Golzari et al[19] showed that placing folded gauze in buccal space in edentulous patients considerably facilitates BMV. In our technique, by pushing the cheek tissue upwards to the mask, it forms an airtight seal around the mask, thus preventing the air leak and adequate external mask fit. It also pulls up the soft palate, thus preventing the obstruction. We have used this technique in a number of our patients. It is important to point out that if mask ventilation remains impossible, the laryngeal mask airway could be used as a rescue devise, especially if there are also difficulties intubating the patient. In summary, BMV in edentulous patients poses a challenge to anaesthesiologist, and by implementing a very minor alteration by pulling the sunken cheek tremendous improvement in BMV can be achieved.
References
1. Ortega R, Mehio AK, Woo A, Hafez DH: Videos in clinical medicine: Positive-pressure ventilation with a face mask and a bag-valve device. N Engl J Med 2007; 357:e4
2. Adnet F: Difficult mask ventilation: An underestimated aspect of the problem of the difficult airway? Anesthesiology 2000; 92:1217-1218.
3. Soleimanpour H, Gholipouri C, Golzari SE, Rahmani F, Sabahi M. Capnography in the emergency department. Emerg Med. 2012; 2:e123.
4. Sokouti M, Montazeri V. Acute nonpenetrating tracheobronchial injuries: What is important in the mortality? J Cardiovasc Thorac Res. 2009; 1:5–8.
5. Soleimanpour H, Sarahrudi K, Hadju S, Golzari SE. How to overcome difficult-bag-mask-ventilation: Recent approaches. Emerg Med. 2012; 2:e116.
6. Conlon NP, Sullivan RP, Herbison PG, Zacharias M, Buggy DJ. The effect of leaving dentures in place on bag-mask ventilation at induction of general anesthesia. Anesth Analg. 2007; 105:370–373. [PubMed: 17646492]
7. Susheela T, Anju G, Reeta S, Kirti K. Edentulous patient and face mask ventilation. Indian J Anesth. 2008; 52:347–348.
8. Magboul M, Ali Magboul. Airway evaluation and assessment for anaesthesia. Internet Journal of Health 2007; 6(1).
9. Thakur S, Thakur JR. Improved anatomical mask for edentulous patients. Indian J Anaesth 2007; 51: 444-445.
10. Conlon NP, Sullivan RP, Herbison PG, Zacharias M, Buggy DJ. The effect of leaving dentures in place on Bag-mask ventilation at induction of general anaesthesia. Anaesth Analg 2007; 105: 370-373.
11. Weiss AM, Lutes M. ACEP News; 2008. Sept, [Last accessed on 23rd July 2014]. Focus on-bag-valve-mask ventilation. Available from: http://www.acep.org/content.aspx?id=40992.
12. Boidin MP. Airway patency in the unconscious patient. Br J Anaesth 1985; 57:306‑310.
13. Nandi PR, Charlesworth CH, Taylor SJ, Nunn JF, Doré CJ. Effect of general anaesthesia on the pharynx. Br J Anaesth 1991; 66:157‑162.
14. Vogel JE, Mulliken JB, Kaban LB. Macroglossia: A review of the condition and a new classification. Plast Reconstr Surg 1986; 78:715‑723.
15. Langeron O, Masso E, Huraux C, Guggiari M, Bianchi A, Coriat P, Riou B: Prediction of difficult mask ventilation. Anesthesiology 2000; 92:1229 –1236.
16. Liang Y, Kimball WR, Kacmarek RM, Zapol WM, and Jiang Y: Nasal ventilation is more effective than combined oralnasal ventilation during induction of general anesthesia in adult subjects. Anesthesiology 2008; 108:998 –1003.
17. Crooke J: The bearded airway. Anaesthesia 1999; 54:500.
18. Stephane X. Racine, Audrey Solis, Nora Ait Hamou, Philippe Letoumelin, David L. Hepner, Sadek Beloucif, Christophe Baillard. Face Mask Ventilation in Edentulous Patients. A Comparison of Mandibular Groove and Lower Lip Placement. Anesthesiology 2010; 112:1190 –1193.
19. Samad EJ Golzari, Hassan Soleimanpour, Hamidreza Mehryar, Shaker Salarilak, Ata Mahmoodpoor, Jafar Rahimi Panahi, et al. Comparison of Three Methods in Improving Bag Mask Ventilation. International Journal of Preventive Medicine 2014; 5: 489-493.
| How to Cite this Article: Thota R S, Baliga P. A unique technique of Bag Mask Ventilation in Edentulous patient: A case report. Journal of Anaesthesia and Critical Care Case Reports July-Sep 2015; 1(1):21-23. |
