Vol 4 | Issue 1 | Jan-Apr 2018 | page: 16-18 | Priyanka Rathi, Arati Ghorpade.
Authors: Abdul Monem [1], Fauzia Anis Khan [2], Sohail Awan [3]
[1] Department of Anaesthesiology, Aga Khan University Hospital
[2] Department of Anaesthesiology, Aga Khan University Hospital
[3] Department of Surgery, Aga Khan University Hospital
Address of Correspondence
Dr. Abdul Monem,
Department of Anaesthesiology,
Aga Khan University
E-mail: abdul.monem@aku.edu
Abstract
Introduction: Vallecular cyst is a rare occurring often encountered incidentally, which may compromise the airway during induction of anesthesia. There is a high risk for cyst rupture and soiling of the airway during manipulation of the airway.
Case Report: We report a case of a young 23-year-old female with a history of difficulty in breathing and swallowing for the past 1½ years. She underwent emergency tracheostomy and excision of some oral swelling 10years back. She was electively booked for excision of the cyst. Various techniques and instruments have been described in the past. We used a tongue depressor to gently push the cyst aside and successfully rail loaded a reinforced endotracheal tube over a gum elastic bougie.
Conclusion: Intubation in a patient with oropharyngeal cyst poses a significant risk in view of complete airway obstruction or aspiration of the contents in case rupture of the cyst. Various techniques for intubation have been reported, either awake or under general anesthesia. We successfully used a tongue depressor to shift the cyst away as an aid for intubation. This technique has so far not been reported in the literature.
Keywords: Vallecular cyst, induction, tongue depressor.
Introduction
Vallecular cyst is a rare cause of airway collapse, which may remain unidentified till induction of general anesthesia. Various methods have been reported to handle such cases. We used atongue depressor and a gum elastic bougieas an aid to intubation in a 23-year-old female.
Case Report
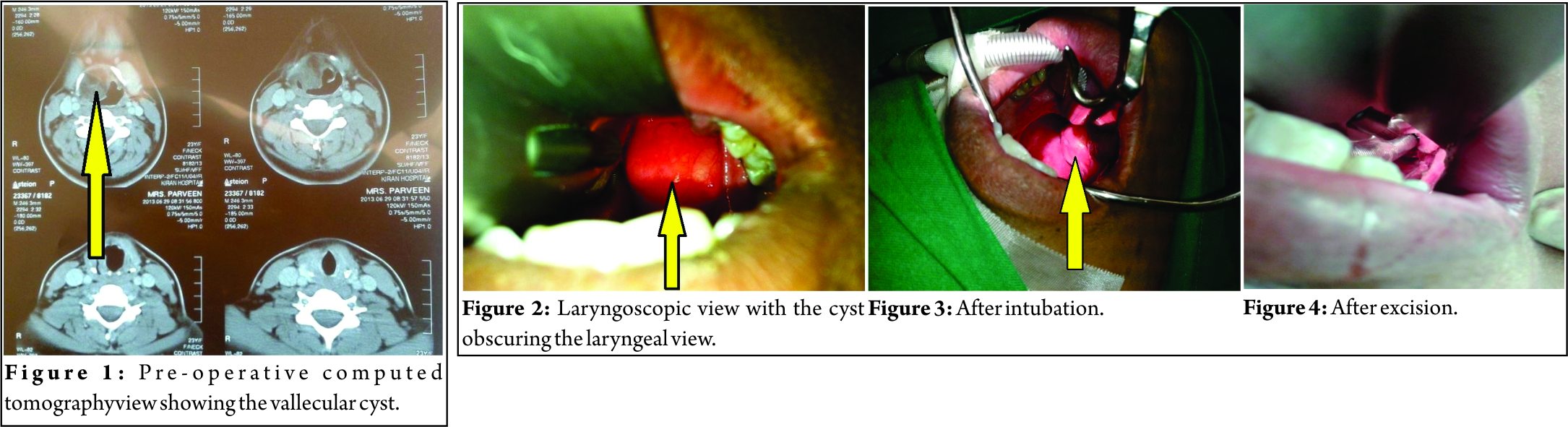
A 23-year-old female presented with a history of snoring and occasional episodes of dysphagia and difficulty in breathing for the past 1½ years. There was no history of change in symptoms associated with achange in body position. She also had a history of palpitations for which she was prescribed propranolol by a general physician. Her thyroid function tests were normal. She had been operated twice before at the age of 10 and 13 years,for a neck swelling which had caused difficulty in breathing and swallowing. She underwent tracheostomy during the first surgery. At the ear, nose, and throat clinic, she underwent an indirect laryngoscopy. A 3 cm × 3 cm swelling was seen arising from the right side of the vallecula. Vocal cords were visible after the fiber-opticscope was negotiated below the swelling. Both cords were normal in anatomy and equally mobile. Her pre-operative computed tomography scan is given in Fig.1.
She was labeled the American Society of Anesthesiologist II with normal laboratory findings including normal thyroid function tests. Shehad a Grade I Mallampati score.
Perioperative course She was planned for excision of cyst under general anesthesia with consent for tracheostomy if required. She underwent inhalational induction with sevoflurane1–8%in 100% oxygen. Careful laryngoscopy was performed using a size 3 Macintosh blade after attaining adequate depth of anesthesia. After the ability to hand ventilate was ensured, intravenous bolus of 100µg fentanyl and 50 mg of propofol was administered. Laryngoscopy revealed a large cyst obscuring the glottic opening.(Fig. 2). A metallic tongue depressor was used to gently press and shift the cyst to the right. A narrow slit like glottic opening then became visible. A size 6 reinforced tracheal tube was then negotiated over a well-lubricated gum elastic bougie without using a muscle relaxant(Fig.3).Tracheal tube was fixed at 20cm mark after confirming bilateral air entry and end-tidal capnography. There was no episode of desaturation during the procedure. Muscle relaxation was provided using atracurium 0.5 mg/kg [1].After inserting a throat pack, the surgeon excised the 3 cm ×3 cm cyst along with the right tonsil(Fig. 4). Two similar cysts were also excised, one through right lateral pharyngotomy and another from the front of the neck(Fig. 5). Patient’s trachea was extubated after insertion of a nasogastric tube. Her post-operative recovery was uneventful and she was discharged 2 days later. Biopsy reported the specimen to be a lipoma.

Discussion
Discussion Congenital laryngeal cysts are rare, with an incidence of 1.82 per 100,000 live births [1].Common sites are 58.2% in the glottic area and 18.3% in the ventricular folds. The remainder waslocated on the aryepiglottic fold (2.2%) and interarytenoid region (0.7%) [2]. These are benign and do not usually cause problems,but unidentified cases are very prone to sudden severe hypoxia and death due to complete airway collapse,especially in children.Adults may present with symptoms of change in voice or dysphagia. Laryngocele and saccular cysts are also rare cause of such symptoms. Laryngoceles cause episodic symptoms as they intermittently fill with air, whereas saccular cysts cause constant symptoms. Children usually present with difficulty in breathing, swallowing, and failure to thrive. Yadav [3] reported hemoptysis as a presenting symptom. Trauma and cyst rupture may lead to aspiration during intubation. Masonand Wark [4] reported two cases of difficult mask ventilation after intravenous induction. Both were found to have vallecularcyst obscuring the glottis view on laryngoscopy. One was intubated after successful aspiration of the cyst by the ENT surgeon. Otherwas intubated with the help of a bougie. McHugh [5] also reported successful intubation with the help of a bougie in an unexpected case of a largeepiglottic cyst. Different methods of airway maintenance have been reported in the anesthetic management of these cases. McKiernan [6] reported blind intubation in a 7-year-old child with the help of smaller tube with double bend on a malleable introducer by pushing an unexpected vallecular cyst to one side. Awake fiber-optic intubation is considered the safest technique in difficult airway management, but this technique may be associated with difficulty to negotiate around the cyst.It may also cause rupture of cyst or traumatic bleed leading to aspiration. Inspite of these disadvantages, it has been successfully used in infants [7]. Ahrens et al. [8] reported intubation of a 3-month-old child with a 2.2 fiber-optic bronchoscope through a laryngeal mask airway. Remifentanil and propofol sedation has been used for fiberoptic intubation in an obstetric patient with a vallecular cyst [9]. It does not increase the risk of aspiration in the mother or leads to sedation in the newborn [10]. Our patient was too anxious to undergo awake fiberoptic intubation. We did not want to administer sedatives in our patient for fear of airway obstruction. As she was able to maintain the airway under inhalational anesthesia, and use of feberoptic laryngoscope was an alternate method that could have been used after inhalational induction. This was our plan B if the use of tongue depressor had failed. Other methods to negotiate the endotracheal tube that has been used include shifting the cyst to one side with the help of a styletted endotracheal tube [11] or lifting of the cyst with a larger Macintosh or a rigid bronchoscopy blade. An angled atraumatic instrument like Mac gills forceps could also be used to shift the cyst away from the intubation path. Although in this case the cyst was thick walled and there was less likelihood of rupture, in case of thin cysts,two wide bore suctions ought to be ready. Shifting the patient to lateral position might help to reopen the complete airway collapse at induction, especially in children [12]. The use of backward,upward,rightward pressure maneuver has been described in a 4 month-old infant [13]. Consent should also be taken for standby tracheostomy. Marsupialization of the vallecular cyst under local anesthesia has also been reported by Pagella et al. [14]. In our case, we used a tongue depressor to push the cyst so that a view of laryngeal inlet could be obtained. By doing so, we were able to intubate the trachea with a size 6 polyvinyl chloride reinforced tracheal tube over a gum elastic bougie. There was some resistance while inserting the tube probably because no muscle relaxant had been used. The use of 4% lignocaine spray might have eased intubation in this patient. The use of tongue depressor in the management of vallecular cyst has not been reported in literature. This simple method was helpful in our case mainly because the cyst was firm and could be displaced laterally. If the cyst had been soft or pedunculated, this might not have been possible. If general anesthesiais chosen as induction technique, inhalational induction with careful laryngoscopic examination should precede attempt at intubation. As the use of muscle relaxants may cause complete airway obstruction, they should be administered after successful endotracheal intubation. Surgical help to perform tracheostomy or puncture of the cyst should be readily available for which consent should be taken before hand
Conclusion
We recommend this simple method of using a tongue depressor as a tracheal intubation aid in anesthetic management of a patient with vallecular cyst.Other atraumatic intubation aids and external laryngeal maneuver might be helpful as well and a gum elastic bougie must be handy in such situations.Consent for emergency tracheostomy should also be taken.
References
1. Pak MW, Woo JK, Van Hasselt CA. Congenital laryngeal cysts: Current approach to management. J LaryngolOtol 1996;10:854-6.
2. Arens C, Glanz H, Kleinsasser O. Clinical and morphological aspects of laryngeal cysts. Eur Arch Otorhinolaryngol 1997;254:430-6.
3. Yadav SP, Sahni JK, Raj B, Chawla RK, Yadav J, Singh B. Laryngeal cyst‐causing haemoptysis. An unusual presentation. Indian J Chest Dis Allied Sci 1986;28:50‐1.
4. Mason DG, Wark KJ. Unexpected difficult intubation. Asymptomatic epiglottic cysts as a cause of upper airway obstruction during anesthesia. Anaesthesia 1987;42:407-12.
5. McHugh P. Cyst of epiglottis (letter). Anaesthesia 1989;44:522.
6. McKiernan EP, Meakin G. Vallecular cysts (letter). Anaesthesia 1988;43:8089.
7. Cheng KS, Ju-Mei Ng, Li HY, Hartigan PM. Vallecular cyst and laryngomalacia in infants: Report of six cases and airway management. AnesthAnalg 2002;95:1248-50.
8. Ahrens B, Lammert I, Schmitt M, Wahn U, Paul K, Gemann B. Life
threatening vallecular cyst in a 3-month-old infant: Case report and literature review. ClinPediatr (Phila) 2004;43:287-90.
9. Prabhu A, ManNally L, Pradhan P, Amin HH. Awake Fibreoptic Intubation in a Pregnant Patient with a Laryngeal Cyst.Int J Periop Ultrasound ApplTechnol 2012;1:74-6.
10. Ovassapian A, Krejcie TC. Awake fiberoptic intubation in a patient at high risk of aspiration. BJA 1989;62:12.
11. Kamble VA, Lilly RB, Gross JB. Unanticipated difficult intubation as a result of an asymptomatic vallecular cyst. Anaesthesiology 1999;3:872-3.
12. Walshe CM, Jonas N, Rohan D. Vallecular cyst causing a difficult intubation. Br J Anaesth 2009;102:565.
13. Namshikar VN, Dukle NV, Sukhthanker DS. Anesthetic management of vallecular cyst excision in an infant: An airway challenge: Case report. Saudi J Anesth 2016;10:356-8.
14. Pagella F, Pusateri A, Matti E, Tinelli G, Benazzo M. Transoral power assisted Marsupializationofvellecular cyst under local anaesthesia. Laryngoscope 2013;123:699-701.
| How to Cite this Article: Monem A, Khan F A, Awan S. Tongue depressor as an intubation aid in a patient with vallecular cyst: A case report. Journal of Anaesthesia and Critical Care Case Reports Sep-Dec 2017; 3(3):. |
