Vol 10 | Issue 1 | January-April 2024 | Page: 01-04 | Maurício Vitor Machado Oliveira, João Paulo Lopes Carvalho Pereira, Lorena Machado Marques Faria, Luiz Fernando Amâncio Pereira de Oliveira, Marina Ayres Delgado
DOI: https://doi.org/10.13107/jaccr.2024.v10.i01.228
Open Access License: CC BY-NC 4.0
Copyright Statement: Copyright © 2024; The Author(s).
Submitted: 07/02/2023; Reviewed: 02/03/2023; Accepted: 18/10/2023; Published: 10/01/2024
Author: Maurício Vitor Machado Oliveira [1], João Paulo Lopes Carvalho Pereira [1], Lorena Machado Marques Faria [1], Luiz Fernando Amâncio Pereira de Oliveira [1], Marina Ayres Delgado [1]
[1] Hospital das clínicas de Belo Horizonte, University of Federal de Minas Gerais, Belo Horizonte, Minas Gerais, Brazil.
Address of Correspondence
Dr. Marina Ayres Delgado,
Hospital das clínicas de Belo Horizonte, Universidade Federal de Minas Gerais. Av Alfredo Balena 110, Santa Efigênia, Belo Horizonte, Minas Gerais, Brasil Cep:30130-100
E-mail: marina.ayres.delgado@gmail.com
Abstract
Background: Acute hepatic failure (ALF) is a disease characterized by rapid deterioration of hepatic function with encephalopathy in a patient without pre-existing liver disease. Bispectral Index (BIS) during the peri-transplant period in patients with fulminant hepatic failure had an important role and its values had a significant correlation with cerebral perfusion. Transcranial Doppler (TCD) can assess changes in cerebrovascular function and has the advantages of being noteworthy, safe, and widely available.
Case report: This is a case report of a serious hepatic encephalopathy occurring during a deceased donor liver transplant (LT) in a patient presenting fulminant hepatitis.
Discussion: We briefly discuss some diagnostic methods highlighting the role and the challenges of the anaesthesiologist in managing this kind of patient in the context of a major surgery.
Keywords: Anaesthesia, Bispectral index monitor, Doppler transcranial ultrasonography, Fulminant liver failure, Hepatic encephalopathy, Intracranial hypertension, Liver transplantation
Introduction
Acute hepatic failure (ALF) is a disease characterized by rapid deterioration of hepatic function with encephalopathy in a patient without pre-existing liver disease due to massive hepatocyte necrosis. In ALF patients, cerebral edema and intracranial hypertension are the most common causes of death (38-81% of cases) [1, 2].
Raised intracranial pressures (ICP) are common in ALF patients. Reperfusion in a new liver graft may also increase cerebral blood flow (CBF), raising ICP in liver transplant recipients. Severe post-transplant brain injury occurred 7.8% of the time and was linked to severe pre-transplant cerebral edema [2, 3].
Patients with liver failure frequently have brain edema, which can lead to serious complications such as cerebral damage. Furthermore, patients with severe hepatic encephalopathy (HE) may have more cerebral damage, which may contribute to delayed and/or incomplete reversal of HE even after LT [2, 4].
We describe a patient whose BIS fell to zero during general anaesthesia, possibly due to cerebral hypoperfusion and the use of a Transcranial Doppler (TDC) as a way to confirm the diagnosis of cerebral hypoperfusion due to a raising ICP.
Case report
C.R.N., 21-year-old, admitted at the hospital with fulminant hepatitis and clinical signs of cerebral edema. undergoing a deceased donor liver transplant. Glasgow coma scale of 3/15 with sedation. Mydriatic and photoreactive pupils. The written informed consent was obtained from the patient’s guardian. Admitted at the operating room already intubated, with an arterial line on the left radial artery and two peripheral vascular access (18G), hemodynamically unstable, in use of norepinephrine (1.1 µg/kg/min). She was then monitored with, electrocardiography, pulse oximeter and the BIS. The Swan Ganz catheter was inserted into the right internal jugular vein and continuous cardiac output, mixed venous saturation and vascular resistances were measured. Preoperative vital signs included blood pressure of 110/55 mmHg, heart hate of 70 beats per minute, oxygen saturation of 96% without oxygen. The patient was mechanically ventilated in the volume control mode, and end-tidal carbon dioxide levels were monitored.
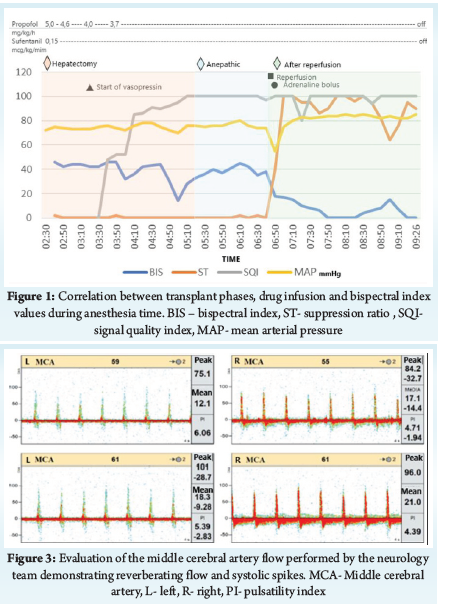
The total venous anaesthesia was performed with sufentanil and propofol, and the infusions were adjusted in order to keep BIS as 40-60. There was no complication during hepatectomy or during anhepatic phases, but after the reperfusion, the BIS values dropped from 40 to zero, stayed at zero with a burst suppression (BSR) rate of 100% (Fig. 1).
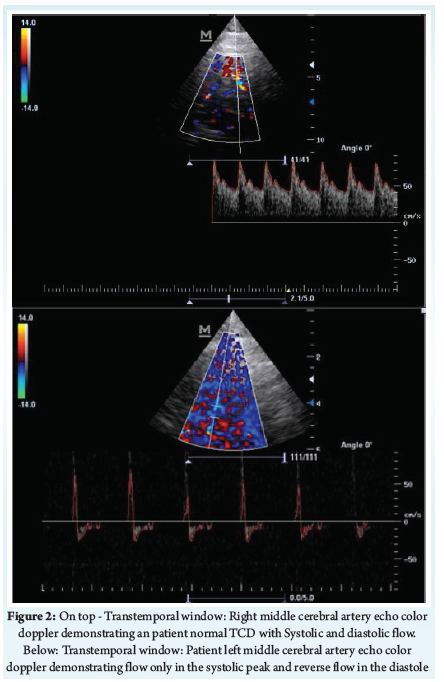
The decrease of BIS was suspected to be the result of decreased cerebral blood flow and the possibility of intracranial hypertension was considered. The measure of the Optic Nerve Sheath Diameter (ONSD) was 5.9mm. The transcranial doppler (TCD) was performed Figure 2, with the evaluation of the middle cerebral artery (MCA), through the transtemporal window, showing a pattern of reverberating flow and systolic spikes. After the suspicion of increased intracranial pressure, 3% NaCl infusion was performed in an attempt to increase serum osmolarity and decrease cerebral edema. A small improvement in the measure of the BIS (18) and in the suppression rate (60%) was observed, however, it was a minor and a momentary improvement.
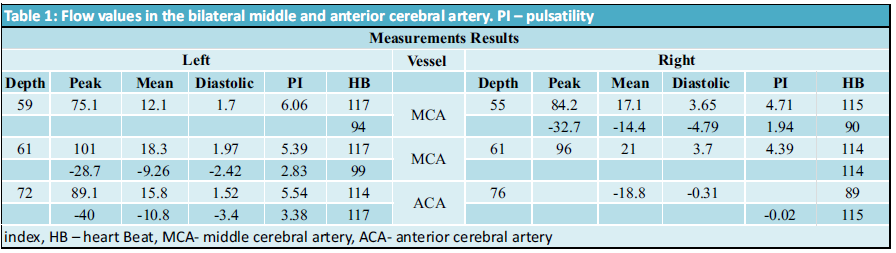
The patient was then transferred to the Intensive Care Unit, with norepinephrine 1.5 µg/kg/min, vasopressin 0,06 UI/min and mean arterial pressure of 85 mmHg. In the ICU, the diagnosis of severe intracranial hypertension and absence of encephalic flow was confirmed by the neurology team Figure 3.
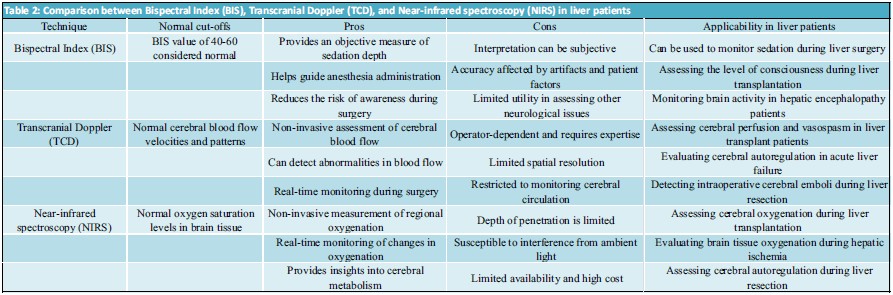
The results are showed in Table 1.
Discussion
The Bispectral index(BIS) was created as a hypnotic drug effect monitor. By analyzing the electroencephalogram, it generates a scale ranging from 0 to 100. (EEG). A BIS of 100 indicates that the subject is awake and responsive. BIS decreases when hypnotics are administered, and a BIS value of 0 represents EEG silence [5]. BIS can drop to nearly zero during surgery due to deep anaesthesia, hypothermia, and cerebral ischemia. Several case reports [1, 3, 6] have identified BIS as an indicator of insufficient cerebral perfusion [7, 8].
In a patient with normal autoregulation, cerebral blood flow (CBF) should be kept constant at 80 mmHg mean arterial blood pressure. However, at this level of mean arterial blood pressure, BIS decreased. A BSR of 100 indicates complete EEG silence, resulting in a BIS value of 0. This implies that a BIS value of 30 indicates EEG suppression when BSR is high. Patients with risk factors, such as a history of ischemic cerebral diseases, may benefit the most from the use of a BIS monitor [7, 9].
Hwang et al evaluated the usability of BIS during the peri-transplant period in patients with fulminant hepatic failure and found that BIS values had a significant correlation with Glasgow coma scale. Furthermore, they proposed that BIS monitoring may be useful in predicting the timing of arousal in patients with fulminant hepatic failure, as well as during peri-transplant management for patients with Hepatic encephalopathy [8].
Dahaba et al evaluated BIS as an early indicator of graft function. They found that recipients with normal graft function had higher BIS after reperfusion under total intravenous anaesthesia with propofol. They speculated that the restoration of hepatic function means the return of cerebral activity, and that the vitality of the transplanted graft could be assessed by BIS [3].
However, as a cerebral perfusion monitor, BIS has some limitations. Only the unilateral frontal cortex is monitored. As a result, the likelihood of false-negative values for other parts of the brain is high [7].
Transcranial Doppler (TCD) is an ultrasound technique that uses blood vessel flow velocities to predict ICP. The relationship between ICP and TCD flow variables was described for the first time in 1988, and it is heavily based on cerebral hemodynamics. Physiologically, as ICP rises, diastolic flow velocity decreases more than systolic flow velocity, resulting in an increased pulse peak between diastole and systole [1, 10, 11].
Transcranial Doppler studies are reliable methods for estimating cerebral autoregulation in both healthy people and patients with chronic and acute liver failure. Doppler is a useful tool in fulminant hepatic failure because it is characterized by an uncoupling between cerebral blood flow and cerebral metabolic rate for oxygen, which is most likely due to a reduction in cerebrovascular resistance [5, 10, 12]. ALF patients had a predominance of cerebral hypo-perfusion, with mean velocities lower than normal and an increased pulsatility index [1].
In this case, knowledge about TCD, especially transtemporal windows with assessment of the flow in the MCA, could suggest the diagnosis of severe intracranial hypertension with the pattern of a reverberating flow and systolic spikes was shown [10-13]. Figure 1 and Figure 2 demonstrated the ”right MCA with alternating flow velocity left MCA with isolated systolic peaks below 50cm/s and others with alternating systolic-diastolic flow”.
In summary, TCD was capable of not only screening but also quantitative assessment of cerebral hemodynamics. It should be noted, however, that fluctuations in PaCO2, MAP, and body temperature, which are common in ALF patients, may change blood vessel elasticity, complicating the interpretation of TCD data and leading to an underestimation of CBF changes [1, 10, 13]. The ultrasound measured optic nerve sheath diameter is a method that can be used to predict the intracranial hypertension during liver transplant [14]. As the ICP increases, this optic nerve The sheath space swells and can be visualized on ultrasound. A typical optic nerve is a variable measured on average by the literature less than 5 mm. A finding greater than this may correlate with a greater ICP make that 20 mm Hg [14, 15]. However, the data on the correct technique and thus the cut-off point necessary for the diagnosis of increased intracranial pressure by this method is quite uncertain. Meta-analyses demonstrate that one of the greatest difficulties in obtaining good evidence in favor of the use of this method is the variability of the methods and measurement techniques of the studies. According to that, TCD was found to be a better predictor of ICP > 14.7 mmHg than ultrasound-measured optic Nerve Sheath Diameter [10, 15].
Near-infrared spectroscopy (NIRS) is a non-invasive technology that has been developed to assess changes in brain oxygenation related to it. NIRS technology is based on the emission of near infrared light (NIR) on the surface of the head and works based on the principle of differential absorption of light in the near infrared spectrum to detect changes in the concentration of oxygen and hemoglobin. Changes in underlying tissue characteristics affect light absorption and scattering, and spectral analysis can be used to obtain information about tissue status and estimated intracranial oxygen saturation, which consequently reflects brain metabolism. In this way, it can also be used to assess changes in brain tissue oxygenation and blood flow [16, 17].
Despite the large increase in studies with NIRS, it still has reduced accuracy due to the effects of scalp and skull injuries, as well as possible pathological changes in baseline saturation, making this technology unreliable for use in all patients and for evaluate absolute values. Within its intended use, it cannot be used to estimate absolute ICP, but rather for the indirect assessment of changes in cerebral perfusion pressure (CPP) and cerebral oxygenation. Therefore, it is plausible to use NIRS to non-invasively assess changes in ICP, but it is more important in a longitudinal use, without the possibility of evaluating an objective number related to the ICP value. More research is needed to better establish the nature of this correlation. Thus, in this case report, NIRS would be useful along with other brain monitoring parameters, helping in the hypothesis of low flow that, together with the clinical history, would increase the suspicion of ICP increase [16, 17].
The table below compares the normal cut-offs, pros, cons, and applicability of three neuromonitoring techniques: Bispectral Index (BIS), Transcranial Doppler (TCD), and Near-infrared spectroscopy (NIRS) in liver patients.
Conclusion
In this case, BIS played an important role in the diagnosis of a cerebral perfusion disorder together with the transcranial Doppler, a rapid, non-invasive, radiation-free method that confirm an imbalance in cerebral flow due to severe intracranial hypertension. In conclusion, we showed the importance of using BIS, the access to ultrasound in the operating room and the anaesthesiologist’s knowledge about neuromonitoring during intraoperative liver transplant.
References
1. Cardim D, Robba C, Czosnyka M, Savo D, Mazeraud A, Iaquaniello C, et al. Noninvasive Intracranial Pressure Estimation With Transcranial Doppler: A Prospective Observational Study. J Neurosurg Anaesthesiol. 2020;32(4):349-53. doi: 10.1097/ANA.0000000000000622. PubMed PMID: 31306262.
2. Spring A, Saran JS, McCarthy S, McCluskey SA. Anaesthesia for the Patient with Severe Liver Failure. Anaesthesiol Clin. 2020;38(1):35-50. Epub 20200103. doi: 10.1016/j.anclin.2019.10.002. PubMed PMID: 32008656.
3. Dahaba AA, Feng ZY, Zhu SM, Bornemann H, Rehak PH, Metzler H. The utility of using bispectral index monitoring as an early intraoperative indicator of initial poor graft function after orthotopic or split-graft liver transplantation. Gut. 2009;58(4):605-6. doi: 10.1136/gut.2008.165118. PubMed PMID: 19299389.
4. Dalal A. Anaesthesia for liver transplantation. Transplant Rev (Orlando). 2016;30(1):51-60. Epub 20150515. doi: 10.1016/j.trre.2015.05.003. PubMed PMID: 26118926.
5. Ardizzone G, Arrigo A, Panaro F, Ornis S, Colombi R, Distefano S, et al. Cerebral hemodynamic and metabolic changes in patients with fulminant hepatic failure during liver transplantation. Transplant Proc. 2004;36(10):3060-4. doi: 10.1016/j.transproceed.2004.11.014. PubMed PMID: 15686694.
6. Bindi ML, Biancofiore G, Esposito M, Meacci L, Bisà M, Mozzo R, et al. Transcranial doppler sonography is useful for the decision-making at the point of care in patients with acute hepatic failure: a single centre’s experience. J Clin Monit Comput. 2008;22(6):449-52. Epub 20081227. doi: 10.1007/s10877-008-9156-6. PubMed PMID: 19112602.
7. Morimoto Y, Monden Y, Ohtake K, Sakabe T, Hagihira S. The detection of cerebral hypoperfusion with bispectral index monitoring during general anaesthesia. Anaesth Analg. 2005;100(1):158-61. doi: 10.1213/01.ANE.0000139347.64944.95. PubMed PMID: 15616071.
8. Hwang S, Lee SG, Park JI, Song GW, Ryu JH, Jung DH, et al. Continuous peritransplant assessment of consciousness using bispectral index monitoring for patients with fulminant hepatic failure undergoing urgent liver transplantation. Clin Transplant. 2010;24(1):91-7. Epub 20091119. doi: 10.1111/j.1399-0012.2009.01148.x. PubMed PMID: 19925461.
9. Kim D, Shin BS, Song I, Han S, Gwak MS, Kim GS, et al. Relationship Between Intraoperative Bispectral Index and Consciousness Recovery in Patients With Hepatic Encephalopathy Undergoing Liver Transplant: A Retrospective Analysis. Transplant Proc. 2019;51(3):798-804. Epub 20190109. doi: 10.1016/j.transproceed.2018.10.031. PubMed PMID: 30979467.
10. Xu W, Gerety P, Aleman T, Swanson J, Taylor J. Noninvasive methods of detecting increased intracranial pressure. Childs Nerv Syst. 2016;32(8):1371-86. Epub 20160628. doi: 10.1007/s00381-016-3143-x. PubMed PMID: 27351182.
11. Alexandrov AV. Extra and Intracranial Waveform Analysis Algorithm, Descriptions, Classifications, and Differential Diagnosis. Journal for Vascular Ultrasound. 2015;39(4):192–202. Epub March 14, 2018. doi: 10.1177/154431671503900403
12. Rasulo FA, Calza S, Robba C, Taccone FS, Biasucci DG, Badenes R, et al. Transcranial Doppler as a screening test to exclude intracranial hypertension in brain-injured patients: the IMPRESSIT-2 prospective multicenter international study. Crit Care. 2022;26(1):110. Epub 20220415. doi: 10.1186/s13054-022-03978-2. PubMed PMID: 35428353; PubMed Central PMCID: PMC9012252.
13. Abdo A, Pérez-Bernal J, Hinojosa R, Porras F, Castellanos R, Gómez F, et al. Cerebral Hemodynamics Patterns by Transcranial Doppler in Patients With Acute Liver Failure. Transplant Proc. 2015;47(9):2647-9. doi: 10.1016/j.transproceed.2015.10.006. PubMed PMID: 26680061.
14. Cardoso FS, Pereira R, Moreno R, Karvellas CJ, Germano N. Optic Nerve Sheath Diameter in Acute Liver Failure: A Prospective Cohort Study. GE Port J Gastroenterol. 2021;28(3):170-8. Epub 20201202. doi: 10.1159/000511646. PubMed PMID: 34056039; PubMed Central PMCID: PMC8138150.
15. Robba C, Santori G, Czosnyka M, Corradi F, Bragazzi N, Padayachy L, et al. Optic nerve sheath diameter measured sonographically as non-invasive estimator of intracranial pressure: a systematic review and meta-analysis. Intensive Care Med. 2018;44(8):1284-94. Epub 20180717. doi: 10.1007/s00134-018-5305-7. PubMed PMID: 30019201.
16. Davies, D. J., Su, Z., Clancy, M. T., Lucas, S. J., Dehghani, H., Logan, A., & Belli, A. (2015). Near-infrared spectroscopy in the monitoring of adult traumatic brain injury: a review. Journal of neurotrauma, 32(13), 933-941.
17. Moraes, F. M. D., & Silva, G. S. (2021). Métodos de monitorização não invasivos da pressão intracraniana: uma revisão crítica. Arquivos de Neuro-Psiquiatria, 79, 437-446.
| How to Cite this Article: Oliveira MVM, Pereira JPLC, Faria LMM, LFAPD, Delgado MA. The Role of Neuromonitoring During Anesthesia of Liver Transplantation: A Case Report. Journal of Anaesthesia and Critical Care Case Reports. January-April 2024; 10(1): 01-04. https://doi.org/10.13107/jaccr.2024.v10.i01.228 |
(Article Full Text HTML) (Download PDF)