Vol 8 | Issue 3 | September-December 2022 | Page: 05-08 | Masami Sato, Munenori Kato, Masahiro Kakuyama
DOI: 10.13107/jaccr.2022.v08i03.206
Author: Masami Sato [1], Munenori Kato [1], Masahiro Kakuyama [1]
[1] Department of Anaesthesia, Kyoto City Hospital, Kyoto, Japan.
Address of Correspondence
Dr. Masami Sato,
Department of Anaesthesia, Kyoto City Hospital, Kyoto, Japan.
E-mail: masami@kb3.so-net.ne.jp
Abstract
Introduction: Pulmonary cement embolism, which is caused by vertebral cement leakage, is a feared but underestimated complication after balloon kyphoplasty. Most pulmonary cement embolism cases are asymptomatic and symptomatic pulmonary cement embolism have been caused by central or peripheral multiple cement emboli.
Case presentation: A 62-year-old man, who underwent three-level thoracolumbar balloon kyphoplasty and pedicle screw fixation for osteoporotic vertebral compression fracture under general anesthesia, experienced hypoxemia postoperatively and dyspnea 1 day after the surgery. Chest computed tomography revealed a small cement embolus in the peripheral pulmonary artery of the right lower lung and confirmed the diagnosis of pulmonary cement embolism. Transthoracic echocardiogram revealed no right heart strain. He was managed successfully under oxygen administration without anticoagulation therapy.
Conclusion: Pulmonary cement embolism after balloon kyphoplasty should be invariably considered as a differential diagnosis when postprocedural dyspnea or hypoxemia occurs. Even a small peripheral cement embolus can induce symptomatic pulmonary cement embolism after balloon kyphoplasty.
Keywords: Pulmonary cement embolism, Balloon kyphoplasty, Pedicle screw fixation, Anticoagulation, General anesthesia.
Introduction
Balloon kyphoplasty (BKP) is a surgical procedure performed for the palliation of painful osteoporotic or cancer-related vertebral compression fractures and has gained popularity because of its minimally invasive procedure performed under local anaesthesia or general anaesthesia. A feared potential complication after BKP is pulmonary cement embolism (PCE) caused by occasional leakage of bone cement into the paravertebral venous system, which drains into the inferior vena cava, and its ultimate lodging in the pulmonary arteries. Most PCE cases are asymptomatic and overlooked because of the lack of pulmonary image screening after surgery. However, some fatal complications can be encountered that require emergent pulmonary thrombectomy or cardiopulmonary resuscitation [1-5]. Postoperative plain chest radiography as a screening tool detects asymptomatic PCE after BKP in 1% of patients [6]. In previous reports, symptomatic PCE after BKP or percutaneous vertebroplasty have been caused by central pulmonary cement embolization or peripheral multiple emboli [1-5, 7-9]. No reports exist regarding symptomatic PCE after BKP induced by only one small peripheral embolus. Herein, we describe a 62-year-old man who experienced hypoxemia and dyspnea induced by a small cement embolus after thoracolumbar BKP and pedicle screw fixation under general anaesthesia. He was diagnosed as having PCE, based on chest computed tomography (CT) that revealed a small cement embolus in the pulmonary artery of the right lower lung and managed through conservative management without anticoagulation therapy.
Case presentation
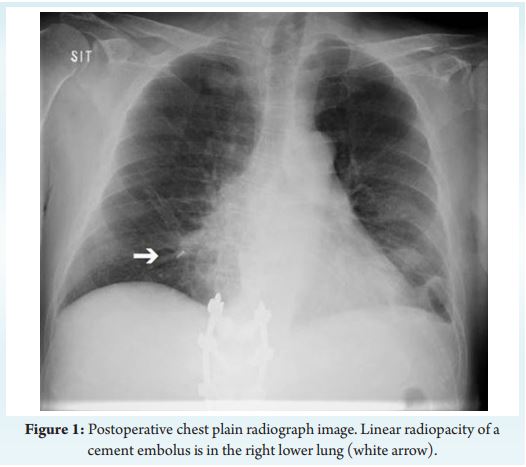
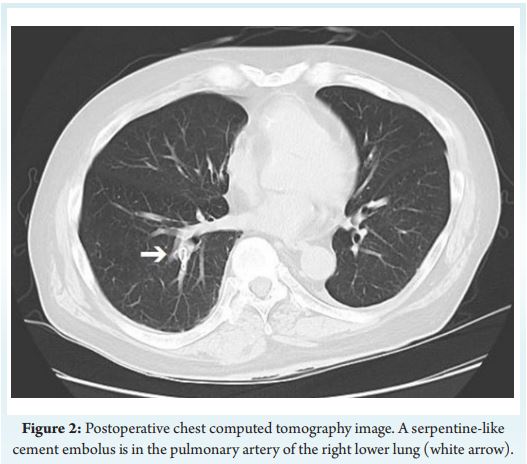
A 62-year-old man (height 164 cm, weight 70 kg) was scheduled to undergo BKP and pedicle screw fixation at T11, T12, and L1, based on the diagnosis of osteoporotic vertebral compression fracture. He was treated with spironolactone and nifedipine for hypertension and atorvastatin for dyslipidemia and did not have a history of respiratory diseases. His pre-anaesthesia percutaneous oxygen saturation (SpO ) 2was 97% on room air. The surgery was performed under general anaesthesia, using propofol, rocuronium, remifentanil and fentanyl. During the surgical procedure, polymethylmethacrylate bone cement (Kyphon HV-R; Medtronic Sofamor Danek Co., Ltd, Memphis, TN, USA) was injected into the aforementioned three vertebral bodies and pedicle screws were placed under fluoroscopic guidance. Cement leakage outside of the vertebral bodies was not observed. The vital signs, including arterial blood gas (ABG), were within the normal ranges throughout the surgery. The operation time was 3 hours 15 minutes. After tracheal extubation, he had slight hypoxemia (ABG: pO = 84.1 mmHg and pCO = 47.7 mmHg with oxygen delivered at 6 2 2L/min via a face mask), but without a complaint of dyspnea. He was transferred to the ward under oxygen administration via a face mask.Three hours after the admission onto the ward, his SpO was 90% on 2the termination of oxygen administration and he needed continuous oxygen. On the first postoperative day, he complained about dyspnea and SpO was around 92% with oxygen via a face mask. Chest plain 2radiography revealed an 8-mm linear radiopacity in the right lower lung field, which suggested PCE (Fig. 1). Chest CT imaging revealed a serpentine-like cement embolus in the peripheral pulmonary artery of the right lower lung (Fig. 2) and cement leakage on the right lateral side of the T11 vertebral body and dorsal side of the L1 vertebral body. Radiologists diagnosed PCE resulting from cement leakage into the paravertebral space and subsequent passage into the venous system and excluded pulmonary thromboembolism. The transthoracic echocardiogram revealed normal left ventricle ejection fraction without right heart strain and no elevated pulmonary arterial pressure. Bronchial asthma and anaphylaxis reaction were ruled out based on his physical finding. At night of the first postoperative day, SpO was 2around 90% with oxygen delivered at 3 L/min via a face mask and he could not sleep because of intermittent breathing difficulty. From the second postoperative day, his subjective respiratory symptom and SpO began to improve under oxygen administration via a face mask. 2On postoperative day 4, SpO kept 93% on room air without 2complaint of dyspnea in the daytime. Supplemental oxygen via a nasal cannula was continued only at night until 6 days after surgery to keep SpO 90% during sleep. Antihypertensive drugs which he had taken 2prior to the surgery was discontinued, because postoperative blood pressure was slightly lower than before surgery. Considering his improvement tendency of respiratory status, small size of the cement embolus and postoperative bleeding risk, anticoagulation therapy was not initiated. Vital signs were carefully monitored in the ward throughout his hospital stay. Although there was no relapse of PCE symptom, his hospital discharge was postponed because of lasting low back pain and prolonged wound healing. He was discharged on postoperative day 30 without further sequelae. He remained stable for 8 months on outpatient follow-up, while chest radiography confirmed the presence of the same cement embolus.
Discussion
The clinical presentation of PCE, which is similar to that of thrombotic pulmonary embolism, varies from dyspnea, being the most common compliant in symptomatic patients, to tachycardia, hypotension, cyanosis, cardiorespiratory arrest, and death. Given the incidence of PCE is low and that most patients with PCE after BKP are asymptomatic, conducting routine postoperative chest radiography is controversial [6]. However, the diagnosis of PCE can be easily confirmed with chest plain radiography or often with CT which can visualize the details of cement emboli matching the pulmonary arteries. Therefore, respiratory symptoms that are indicative of PCE reasonably warrant chest radiography or CT, which would prevent a delay in the diagnosis and management of PCE. Postoperative close vitals monitoring to detect the development of PCE is also mandatory, especially after general anaesthesia when a variety of factors, including the influence of anesthetics, may induce hypoxemia. In our patient, chest plain radiography in the operating room may have been indicated before his transfer to the ward to investigate the cause of his slight hypoxemia, although without a complaint of dyspnea.Our patient experienced moderate dyspnea from the first to fourth postoperative day in addition to hypoxemia, although the cement embolus in the peripheral pulmonary artery was small. On the contrary, Bliemel et al. reported a case of a 69-year-old woman in which chest radiograph after BKP confirmed the diagnosis of PCE by showing numerous cement emboli in both lungs, although she remained clinically asymptomatic [6]. Based on a review study on bone cement implantation syndrome, the degree of embolic load in pulmonary circulation is not correlated with the severity of hypotension or hypoxemia [10]. In addition to simple mechanical obstruction of pulmonary arteries from emboli, a possible mechanism of bone cement implantation syndrome is that biochemical mediators released from emboli or stimulated endothelium cause an increase in pulmonary vascular resistance [10]. Rahimizadeh et al. reported a case of cardiopulmonary arrest induced by PCE from multiple large central emboli on the next day of the pedicle screw cement augmentation [3]. They successfully extubated the patient 24 hours later with conservative measures. The reason for the drastic recovery within a short period, while pulmonary arteries remained blocked by cement emboli, would be that mediator-related temporal vasoconstriction was involved in the onset of PCE symptoms. Our patient’s symptom would also be attributed to the ventilation-perfusion mismatch primarily by pulmonar y vasoconstriction induced by biochemical mediator, rather than mechanical obstruction induced by a small embolus. When respiratory distress occurs after vertebral cement augmentation procedures, it is necessary to keep in mind that even a small peripheral cement embolus may be the cause of symptomatic PCE, while taking other respiratory diseases into consideration as differential diagnosis. In our case, close respiratory monitoring including ABG analysis at intensive care unit should have been considered without being confused by the size of the cement embolus on the next day of the surgery when the patient showed dyspnea.Intraoperative cement leakage into the paravertebral space causes PCE and tends to be induced by applying high intravertebral pressure when injecting bone cement [2, 6, 11]. There are two types of vertebral cement augmentation procedures; BKP and percutaneous vertebroplasty. BKP is safer than percutaneous vertebroplasty, because cement injection during BKP exerts lower intravertebral pressure than during percutaneous vertebroplasty [6, 11, 12]. Therefore, the incidence of symptomatic and asymptomatic PCE is lower with BKP than with percutaneous vertebroplasty (0.67% vs. 3.3%), based on CT examinations findings conducted 1 month after surgery [11]. However, pedicle screw fixation combined with BKP increase the pressure of cement injected into the vertebral body and subsequently would be associated with high cement leakage rate [2, 3]. Patients who have fractured thoracic vertebrae rather than lumber vertebrae, or who have three or more involved vertebrae, or who have low viscous cement applied during the surgery have a risk of developing PCE after vertebral cement augmentation procedures [2, 11]. The procedure used for our patient, three-level thoracolumbar BKP with pedicle screw fixation, had the risk of PCE, although a high viscous cement was applied. The treatment for PCE depends on symptoms severity and location and size of the embolus. Although reported treatments include observation with clinical follow-up, supportive care, anticoagulation therapy, and retrieval of the cement embolus, no clear standardized management of symptomatic PCE exists [1, 12]. Our symptomatic peripheral embolism is recommended to be treated with heparinization initially, followed by 3-6 months of consecutive warfarin therapy, based on the proposed algorithm for treatment choice of PCE by Krueger et al. [12]. In fact, Patel et al. reported a case of symptomatic PCE induced by several peripheral emboli and its successful treatment with anticoagulants for 6 months [8]. Of course, anticoagulation therapy reduces the risk of progressive thrombus formation on the embolic material, but it cannot release the obstruction by the cement or reduce the right ventricle afterload. Routine use of anticoagulants for treatment of symptomatic PCE, following the standard treatment guideline for thromboembolic pulmonary embolism, does not get a conclusion [1, 7, 9, 13]. Investigators have reported that incidentally detected PCE has no significant effects on long-term mortality, although patients with PCE were observed without any treatment [14]. In our patient, hypoxemia and dyspnea were induced by a small peripheral embolus without hemodynamic instability and PCE was diagnosed on the next day of the surgery along with postoperative bleeding risk due to anticoagulant use. Therefore, we chose conservative management without initiating anticoagulation therapy. Our case illustrates a variation on the management of symptomatic PCE by a small peripheral embolus, however, additional studies are needed to investigate any long-term complications of PCE in patients under conservative therapy without anticoagulation therapy.
Conclusion
We experienced a case of symptomatic PCE caused by a small peripheral embolus after BKP and pedicle screw fixation. When respiratory distress occurs postoperatively, PCE should be invariably considered as a differential diagnosis, even if the cement embolus was small. Conservative management without anticoagulation therapy can be an option for symptomatic PCE caused by a small peripheral embolus.
References
1. Barakat AS, Owais T, Alhashash M, Shousha M, Saghir HE, Lauer B, et al. Presentation and management of symptomatic central bone cement embolization. Eur Spine J. 2018;27(10):2584-92.
2. Janssen I, Ryang YM, Gempt J, Bette S, Gerhardt J, Kirschke JS, et al. Risk of cement leakage and pulmonary embolism by bone cement-augmented pedicle screw fixation of the thoracolumbar spine. Spine J. 2017;17(6):837-44.
3. Rahimizadeh A, Hassani V, Soufiani H, Rahimizadeh A, Karimi M, Asgari N. Symptomatic pulmonary cement embolism after pedicle screw polymethylmethacrylate cement augmentation: A case report and review. Surg Neurol Int. 2020;11:18.
4. Rothermich MA, Buchowski JM, Bumpass DB, Patterson GA. Pulmonary cement embolization after vertebroplasty requiring pulmonary wedge resection. Clin Orthop Relat Res. 2014;472(5):1652-7.
5. Stricker K, Orler R, Yen K, Takala J, Luginbühl M. Severe hypercapnia due to pulmonary embolism of polymethylmethacrylate during vertebroplasty. Anesth Analg. 2004;98(4):1184-6.
6. Bliemel C, Buecking B, Struewer J, Piechowiak EI, Ruchholtz S, Krueger A. Detection of pulmonary cement embolism after balloon kyphoplasty: should conventional radiographs become routine? Acta Orthop Belg. 2013;79(4):444-50.
7. Idiculla PS, Rajdev K, Pervaiz S, Cinelli M, Habib S, Siddiqui A, et al. Cement pulmonary embolism after balloon kyphoplasty. Respir Med Case Rep. 2019;28:100887.
8. Patel Z, Sangani R, Lombard C. Cement pulmonary embolism after percutaneous kyphoplasty: an unusual culprit for non-thrombotic pulmonary embolism. Radiol Case Rep. 2021;16(11):3520-5.
9. Waler AR, Sanchez KJ, Parikh AA, Okorie ON. A case of pulmonary cement embolism managed through symptomatic treatment. Case Rep Crit Care. 2020:2425973.
10. Donaldson AJ, Thomson HE, Harper NJ, Kenny NW. Bone cement implantation syndrome. Br J Anaesth. 2009;102(1):12-22.
11. Zou D, Dong S, Du W, Sun B, Wu X. Risk factor analysis of pulmonary cement embolism during percutaneous vertebroplasty or kyphoplasty for osteoporotic vertebral compression fractures. J Orthop Surg Res. 2021;16(1):312.
12. Krueger A, Bliemel C, Zettl R, Ruchholtz S. Management of pulmonary cement embolism after percutaneous vertebroplasty and kyphoplasty: a systematic review of the literature. Eur Spine J. 2009;18(9):1257-65.
13. Mansour A, Abdel-Razeq N, Abuali H, Makoseh M, Shaikh-Salem N, Abushalha K, et al. Cement pulmonary embolism as a complication of percutaneous vertebroplasty in cancer patients. Cancer Imaging. 2018;18(1):5.
14. Kang HR, Kim TH, Chung CK, Lee CH. The impact of incidental pulmonary cement embolism on mortality risk. J Thromb Thrombolysis. 2020;49(3):468-74.
| How to Cite this Article: Sato M, Kato M, Kakuyama M | Symptomatic Pulmonary Cement Embolism after Balloon Kyphoplasty and Pedicle Screw Fixation Caused by a Small Peripheral Embolus- A Case Report | Journal of Anaesthesia and Critical Care Case Reports | September-December 2022; 8(3): 00-00. |