Vol 5 | Issue 2 | May-Aug 2019 | page: 4-5 | Tuhin Mistry, Hetal Kumar Vadera, Shiv Kumar Singh
Authors: Tuhin Mistry [1], Hetal Kumar Vadera [2], Shiv Kumar Singh [3]
[1] Department of Onco-Anaesthesiology, Dr B. R. A. IRCH, AIIMS, New Delhi, India
[2] Department of Anaesthesiology, Sterling Hospital, Rajkot, Gujarat, India
[3] Department of Anaesthesiology, Royal Liverpool University Hospitals, Prescot Streets, Liverpool, UK.
Address of Correspondence
Dr. Tuhin Mistry,
Department of Onco-Anaesthesiology, Dr B. R. A. IRCH, AIIMS, New Delhi, India;
E-mail: tm.tuhin87@gmail.com
Technical Note
Dear Editor,
There is often confusion amongst the anaesthetists about subcostal transversus abdominis plane (SCTAP) and subcostal approach to TAP block (SATAP). SCTAP, also known as“oblique subcostal” TAP block, is used to produce reliable analgesia for the supra-umbilical abdominal procedures. For the SCTAP, a long needle of 100 to 150 mm length is introduced in plane with a linear ultrasound probe positioned perpendicular to the abdominal wall, directed parallel to the costal margin but oblique to the sagittal plane.[1] The needle insertion starts at a point near the xiphoid process and the local anesthetic(LA)is initially deposited between transversus abdominis and the rectus abdominis muscles, or between the rectus muscle and the posterior rectus sheath if transversus is not behind rectus at that level, basically a rectus sheath block in the upper quadrant. The needle is then directed inferolaterally to progressively distend the transversus abdominis plane parallel to the costal margin blocking the intercostal nerves as they emerge to run into the transversus abdominis plane. Two injection points may be technically easier to ensure that LA is deposited along the plane.
Ultrasound guided SCTAP as described by Peter Habbard is considered a better alternative than posterior TAP block toprovide postoperative analgesia for laparoscopic cholecystectomy.[2] It was also found to be comparable with quadratus lumborum block in decreasing postoperative pain scores and analgesic consumptionwith higher patient satisfaction.[3]However, not everyone has access to the ultrasound machines in the operation theatre. We describe a novel anatomical landmark guided loss of resistance(LOR) technique for SCTAP block that can be performed to provide perioperative analgesia. This technique is combination of rectus sheath block (RSB) and subcostal approach to TAP (SATAP) block.
LOR guided SCTAP blocks can be performed preoperatively in the holding area, after induction of anaesthesia in the operating room, or postoperatively after the surgery is completed. The challenge of performing the SCTAP block in the post-opperiod is the distortion of the abdominal musculature and TA plane caused by surgery.
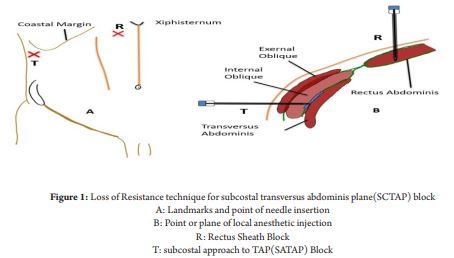
Aim of this block is to deposit LAat two points, first point is the RSBin the upper quadrant of the abdomen and then, in the fascial plane between the transversus abdominis and internal oblique muscles under the costal margin (SATAP).Figure 1 depicts the landmark used toperform theblocks.
After appropriate skin preparation, a short bevel or a blunt needle is connected to a syringe with 20 mLs of LA. The first injection is done in the upper quadrant of the abdomen, the point of injection is 3-4 cms below the xiphoid and 3-4cms lateral to the linea alba.[Figure 1.A] After aseptic precautions, a 50 -80 mm blunt tipped needle is introduced through the skin. Once the skin barrier is breached, the needle is withdrawn back so that the tip lies just under the skin,it is then advanced till resistance is felt over the anterior rectus sheath. The needle is “bounced” over this fascia and advanced further to feel a distinct “pop” as the needle passes through the anterior rectus sheath. The needle is then advanced further through the rectus muscle till resistance over the posterior rectus sheath is felt and a “bounce” is demonstrated. This is the pointof injection; needle is not advanced any further and 10-15mLs of LA (0.25% Bupivacaine or 0.2% Ropivacaine) is deposited.[Figure 1.B]
For the SATAP, following aseptic precautions, a short bevel or blunt needle is introduced one finger breadth (2-3 cm) below the costal margin in the mid-axillary line, almost perpendicular to the skin.[Figure 1.A] Once the skin barrier is breached, the needle is withdrawn back so that the tip lies just under the skin. The needle is then advanced through the external oblique muscle and the first “pop” sensation is felt when the needle enters the plane between the external oblique (EO) and internal oblique (IO) muscles. We tend to actively look for a “bounce” of the blunt tipped needle on the fascia before advancing it to feel the “pop” as the needle pierces the strong fascia. Further advancement of the needle through the internal oblique muscle and then the fascia underneath it,results in a second “pop” and the tip of the needle lying in the TAP, the neurovsacular plane where the LA need to be deposited.[Figure 1.B] At this point, after careful aspiration, LA is injected in 5 mL aliquots. A volume of 15-20 ml of 0.25% (levo) bupivacaine or 0.2% ropivacaine with or without adjuvants can be used for somatic analgesia depending upon the surgicalrequirements. While using bilateral blocks, it is important to keep in mind the toxic limits of the LA.
Although these blocks are simple, effective and easy to perform, a randomized controlled trial is required to validate its efficacy, safety, and reliability compared to ultrasound guided techniques.
References
1. Hebbard P. Subcostal transversus abdominis plane block under ultrasound guidance. Anesthesia & Analgesia. 2008;106(2):674-5
2. Bhatia N, Arora S, Jyotsna W, Kaur G. Comparison of posterior and subcostal approaches to ultrasound-guided transverse abdominis plane block for postoperative analgesia in laparoscopic cholecystectomy. J Clin Anesth. 2014;26(4):294-9.
3. Baytar Ç, Yılmaz C, Karasu D, Topal S. Comparison of Ultrasound-Guided Subcostal Transversus Abdominis Plane Block and Quadratus Lumborum Block in Laparoscopic Cholecystectomy: A Prospective, Randomized, Controlled Clinical Study. Pain Res Manag. 2019:2815301.
| How to Cite this Article: Mistry T, Vadera H K, Singh S K. Subcostal Transversus Abdominis Plane block: Loss of Resistance Technique. Journal of Anaesthesia and Critical Care Case Reports May-Aug 2019; 5(2): 4-5. |
(Full Text HTML) (Download PDF)
.