Vol 2 | Issue 2 | May – Aug 2016 | page:5-8 | Patrick Tunney, Nevin K Chinnan
Author: Patrick Tunney[1], Nevin K Chinnan [1].
[1] Dubbo Base Hospital, NSW- 2430.
Address of Correspondence
Dr. Nevin Kollannoor Chinnan
MD, DNB, FCICM
Consultant Intensivist
Dubbo Base Hospital
NSW-2430
Email: nevinkc2001@yahoo.com
Serum Lactate in Intensive Care: Practical Points and Pitfalls
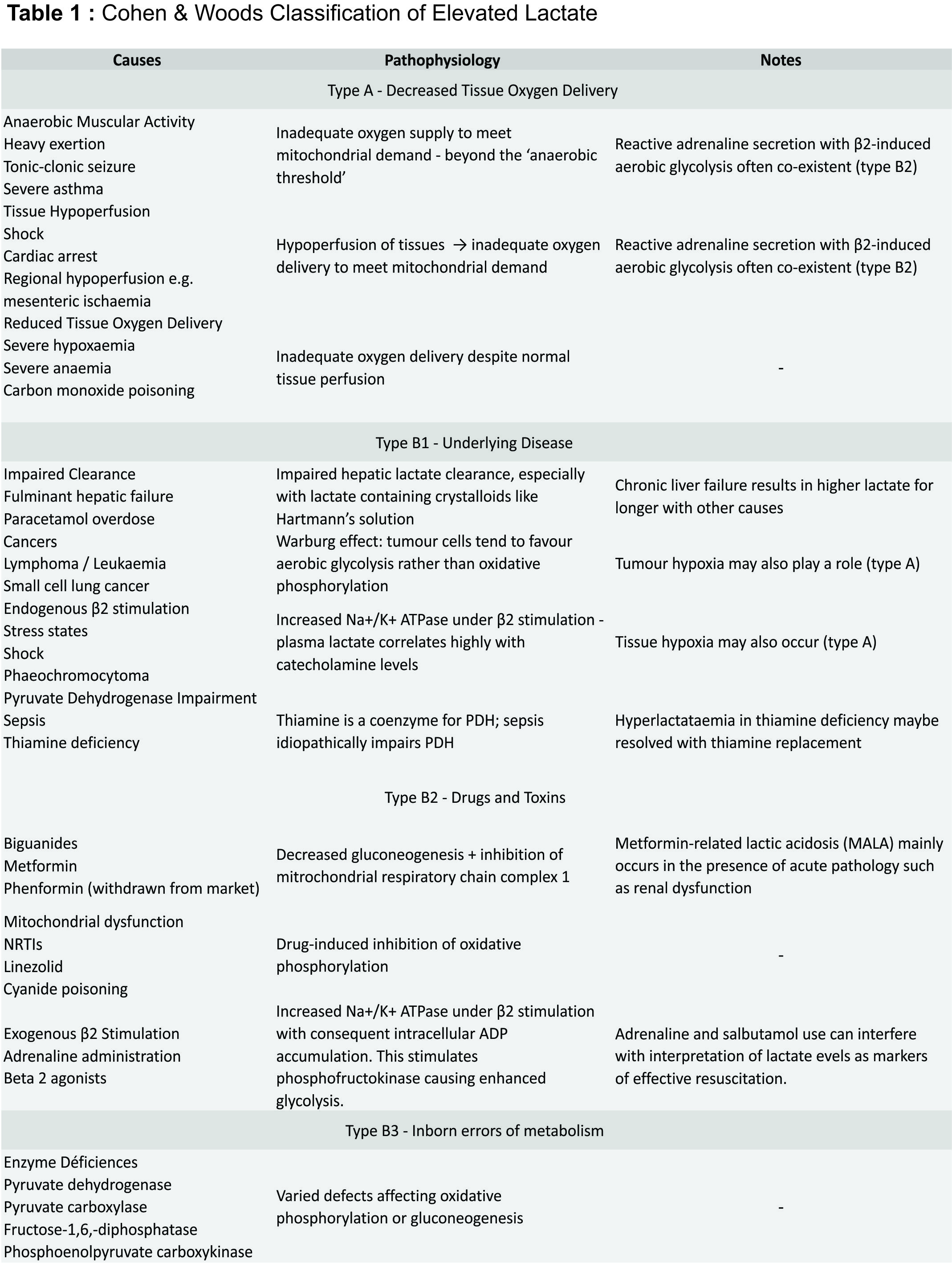
In clinical practice, serum L-lactate has become an important marker of prognosis and resolution of diverse critical illnesses, including sepsis and septic shock. The newly released Sepsis-3 criteria include serum lactate as diagnostic criteria for septic shock [1]. Here, we summarise current knowledge regarding the use of lactate in clinical practice and investigates the role of lactate in a post-SIRS era. D-lactate (an isomer of L-lactate) causes a distinct clinical entity of different aetiology which is not included here; henceforth, L-lactate will be referred to as lactate. Pyruvate is formed mainly (65%) from glucose via glycolysis, though a small amount (16-20%) is produced from metabolism of alanine (Figure 1) [2]. In the presence of oxygen and adequate mitochondrial capacity, pyruvate is then converted by pyruvate dehydrogenase complex to acetyl CoA, which enters the Krebs cycle and undergoes mitochondrial oxidative phosphorylation. In the absence of adequate oxygen or in the presence of excessive glycolysis, pyruvate is unable to undergo oxidative phosphorylation and is instead shunted into lactate by the enzyme lactate dehydrogenase. Lactate is metabolised primarily (60%) by the liver through gluconeogenesis and oxidation. Under resting conditions ~5% of lactate is metabolised by the kidney; in hyperlactataemia the kidney metabolises up to 25-30% of lactate [3]. The remainder is metabolised by myocytes. Lactate accumulation may be associated with acidosis, especially at higher serum lactate concentrations; acidic conditions impair the liver’s ability to process lactate but increase renal lactate metabolism [3]. The acidosis associated with lactate is a high anion gap metabolic acidosis as lactate is an unmeasured anion. Elevated serum lactate is an indicator of production/consumption mismatch. The Cohen and Woods classification (Table 1) has long been used to differentiate between causes of hyperlactataemia, with type A representing causes due to decreased tissue oxygen supply and type B including all other causes. This classification belies the complexity of lactate pathophysiology, with multiple processes often present in one patient. Currently, two principle methods of serum lactate estimation are in clinical use. The lactate dehydrogenase (LDH) method in use by most laboratories relies on the spectrophotometric measurement on light absorption before and after addition of LDH, reflecting the amount of NADH formed as lactate is metabolised. The lactic acid oxidase method employed by most point-of-care (POC) devices (including iSTAT and Radiometer machines) uses amperometry to measure current produced by hydrogen peroxide formation (from lactate) at a platinum anode. The most significant error with the latter method is the false positive produced by glycolate, a metabolite of ethylene glycol. The lactate gap is the difference between the results of these two methods; an elevated lactate gap is suggestive of ethylene glycol poisoning [4, 5].
Lactate now makes up part of the definition for septic shock under Sepsis-3 [1]. These definitions reflect a change in the current sepsis paradigm, with removal of the SIRS criteria and the addition of the Sequential Organ Failure Assessment (SOFA) to quantify multiorgan dysfunction. Sepsis-3 also includes the quickSOFA criteria as a screening tool for sepsis. Septic shock under the new consensus definitions is the presence of sepsis (infection + SOFA ≥2), persistent hypotension requiring vasopressors to maintain MAP ≥65, and serum lactate >2mmol/L. Patients meeting these criteria have an estimated mortality of 42% [1]. Elevated lactate in sepsis has traditionally been attributed to anaerobic metabolism in the setting of macrocirculatory and microcirculatory dysfunction. Hypotension and hypoperfusion occur at a systemic level due to vasodilatation, while microcirculatory shunting occurs at a capillary level due to arteriolar hyporesponsiveness, reduction in perfused capillaries and venular inflammation [6, 7]. However, there is increasing evidence that elevated lactate in patients with septic shock is multifactorial. Pyruvate production and oxidation are infact greater in severely septic patients when compared to healthy volunteers, suggesting that tissue hypoxia plays only a minor role [8]. Adrenaline-induced ß2 activation is also likely to be involved in sepsis. Activation of ß2-adrenoceptors activates of Na+/K+ ATPase, a transmembrane protein that hydrolyses ATP to ADP in order to balance sodium and potassium concentration gradients. The ADP accumulation stimulates phosphofructokinase activity, resulting in increased glycolysis and lactate accumulation [9,10]. Idiopathic pyruvate dehydrogenase (PDH) impairment also plays a role in hyperlactataemia of sepsis [11], which may in some cases be compounded by PDH impairment due to thiamine deficiency [12].
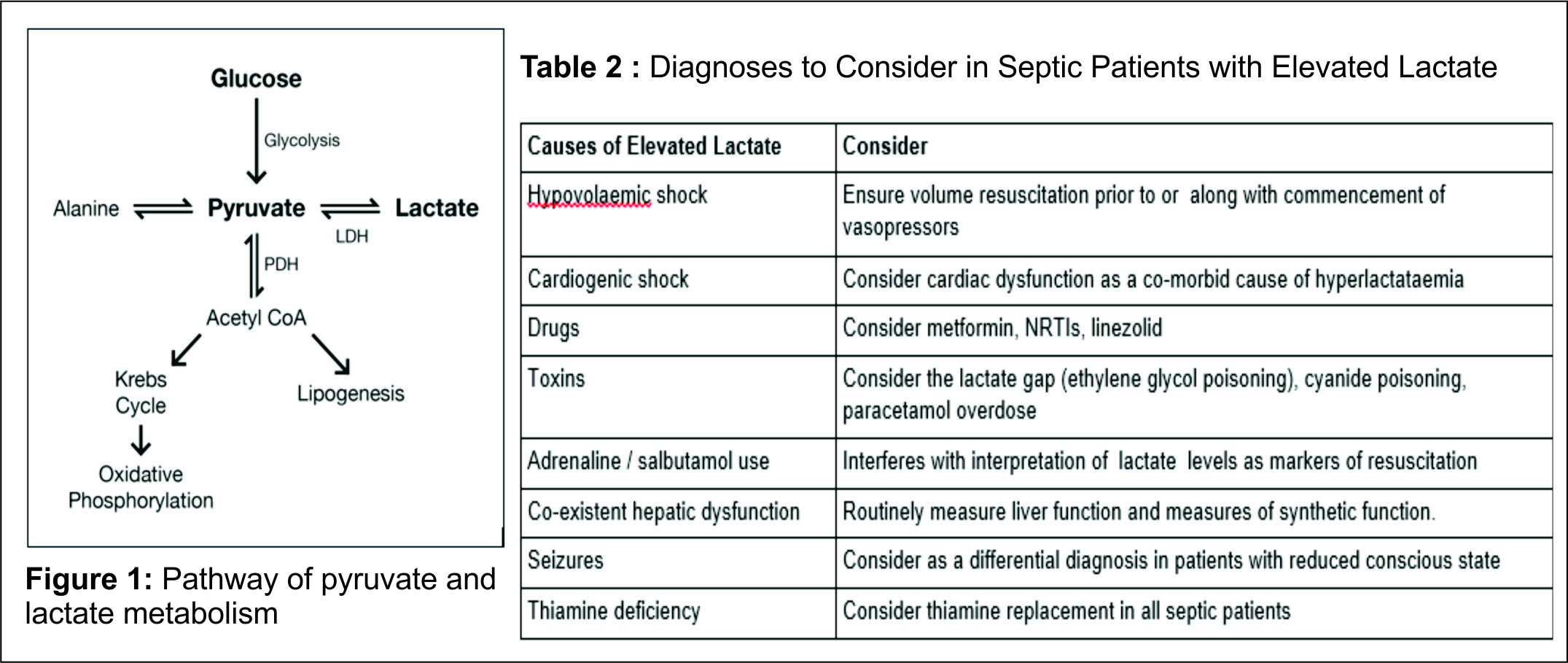
Decreased lactate clearance may occur in sepsis, both idiopathically [13] and as a result of pre-existing liver disease [14]. Lactate is an independent predictor of mortality in sepsis, with serum lactate ≥4mmol/L associated with 28-38% mortality [15,16]. Despite aggressive resuscitation of shocked patients, the subsets of patients who have persistently elevated lactate concentrations continue to develop multiple organ dysfunction and higher mortality [17]. There is no significant difference in measures of tissue oxygenation (VO2 and DO2) between survivors and non-survivors of sepsis [18], suggesting that lactate is better placed as a marker of overall prognosis rather than a marker of tissue hypoxia. Lactate clearance is also a useful marker of resolution in sepsis; high lactate clearance at 6 hours is associated with improvement in inflammatory markers, markers of organ dysfunction (including SOFA score) and overall outcome [19]. The Surviving Sepsis campaign guidelines currently suggest normalisation of lactate as a goal of resuscitation [20]. Elevated serum lactate may be caused by a wide variety of processes, and often many processes co-exist in one patient. With Sepsis-3, lactate will be used increasingly as a marker of prognosis in sepsis and septic shock, and it is important to consider that the hyperlactataemia (Table 1) in these cases is multifactorial in its aetiology. In patients with suspected sepsis and elevated lactate it is wise to consider co-existent causes of hyperlactataemia in order to improve patient outcomes; this is especially important in patients whose markers of sepsis are improving.
References
1. Singer M, Deutschman CS, Seymour CW, Shankar-Hari M, et al. The third international consensus definitions for sepsis and septic shock (sepsis-3). Jama 2016 ;315(8):801-10.
2. Perriello G, Jorde R, Nurjhan N, Stumvoll M, et al. Estimation of glucose-alanine-lactate-glutamine cycles in postabsorptive humans: role of skeletal muscle. American Journal of Physiology-Endocrinology and Metabolism 1995;269(3):E443-50.
3. Bellomo R. Bench-to-bedside review: lactate and the kidney. Critical Care 2002;6(4):1.
4. Brindley PG, Butler MS, Cembrowski G, Brindley DN. Falsely elevated point-of-care lactate measurement after ingestion of ethylene glycol. Canadian Medical Association Journal 2007;176(8):1097-9.
5. Venkatesh B, Morgan T, Garrett P. Measuring the lactate gap. The Lancet 2001;358(9295):1806.
6. Spronk PE, Zandstra DF, Ince C. Bench-to-bedside review: sepsis is a disease of the microcirculation. Critical care 2004 ;8(6):1.
7. Lush CW, Kvietys PR. Microvascular dysfunction in sepsis. Microcirculation 2000;7(2):83-101.
8. Gore DC, Jahoor F, Hibbert JM, DeMaria EJ. Lactic acidosis during sepsis is related to increased pyruvate production, not deficits in tissue oxygen availability. Annals of surgery 1996;224(1):97.
9. Levy B, Gibot S, Franck P, Cravoisy A, et al. Relation between muscle Na+ K+ ATPase activity and raised lactate concentrations in septic shock: a prospective study. The Lancet 2005;365(9462):871-5.
10. McCarter FD, Nierman SR, James JH, Wang L, et al. Role of skeletal muscle Na+–K+ ATPase activity in increased lactate production in sub–acute sepsis. Life sciences 2002;70(16):1875-88.
11. Vary TC. Sepsis-induced alterations in pyruvate dehydrogenase complex activity in rat skeletal muscle: effects on plasma lactate. Shock 1996;6(2):89-94.
12. Donnino MW, Carney E, Cocchi MN, Barbash I, et al. Thiamine deficiency in critically ill patients with sepsis. Journal of critical care 2010;25(4):576-81.
13. Levraut J, Ciebiera JP, Chave S, Rabary O, et al. Mild hyperlactatemia in stable septic patients is due to impaired lactate clearance rather than overproduction. Am J RespirCrit Care Med. 1998; 157(4 Pt 1):1021-6.
14. Moreau R, Hadengue A, Soupison T, Kirstetter P, et al. Septic shock in patients with cirrhosis: hemodynamic and metabolic characteristics and intensive care unit outcome. Critical care medicine 1992;20(6):746.
15. Shapiro NI, Howell MD, Talmor D, Nathanson LA, et al. Serum lactate as a predictor of mortality in emergency department patients with infection. Annals of emergency medicine 2005;45(5):524-8.
16. Trzeciak S, Dellinger RP, Chansky ME, Arnold RC, et al. Serum lactate as a predictor of mortality in patients with infection. Intensive care medicine 2007;33(6):970-7.
17. Bakker J, Gris P, Coffernils M, Kahn RJ, et al. Serial blood lactate levels can predict the development of multiple organ failure following septic shock. The American journal of surgery 1996;171(2):221-6.
18. Bakker J, Coffernils M, Leon M, Gris P, et al. Blood lactate levels are superior to oxygen-derived variables in predicting outcome in human septic shock. Chest 1991;99(4):956-62.
19. Nguyen HB, Rivers EP, Knoblich BP, Jacobsen G, et al. Early lactate clearance is associated with improved outcome in severe sepsis and septic shock. Critical care medicine 2004;32(8):1637-42.
20. Dellinger RP, Levy MM, Rhodes A, et al. Surviving sepsis campaign: international guidelines for management of severe sepsis and septic shock: 2012. Crit Care Med. 2013;41(2):580-637.
| How to Cite this Article:Tunney P, Chinnan NK. Serum Lactate in Intensive Care: Practical Points and Pitfalls. Journal of Anaesthesia and Critical Care Case Reports May-Aug 2016; 2(2): 5-8. |