Vol 4 | Issue 1 | Jan-Apr 2018 | page: 38-39 | Deepak Madankar, Neelesh Mathankar
Authors: Dr Deepak Madankar [1], Dr Neelesh Mathankar [1]
[1] Department of Anaesthesiology and Pain Medicine, Meditrina Institute of Medical Sciences, Nagpur, Maharashtra, India.
Address of Correspondence
Dr. Deepak P Madankar
Meditrina Institute of Medical Sciences 278, Central Bazar Road
Ramdaspeth, Nagpur (MS) India.
E-mail: deepakmadankar30@gmail.com
Abstract
Scavenging port obstruction in anesthesia machine can cause increased pressure within the circuit and can lead to extreme physiological disruptions. We present an unusual case scenario where scavenging port obstruction led to increased airway pressures and reduced tidal volume.
Introduction
It is a well-known fact that obstruction to the expired gas flow in a breathing system will cause building up of pressure within the circuit and result in physiological disruptions such as barotrauma, unstable hemodynamics, and other serious complications including the risk of pneumothorax. Literature highlights various causes of obstruction of gaseous outlet or scavenging port [1, 2, 3, 4, 5]. We report an unusual cause of obstruction to the scavenging system.
Case Report
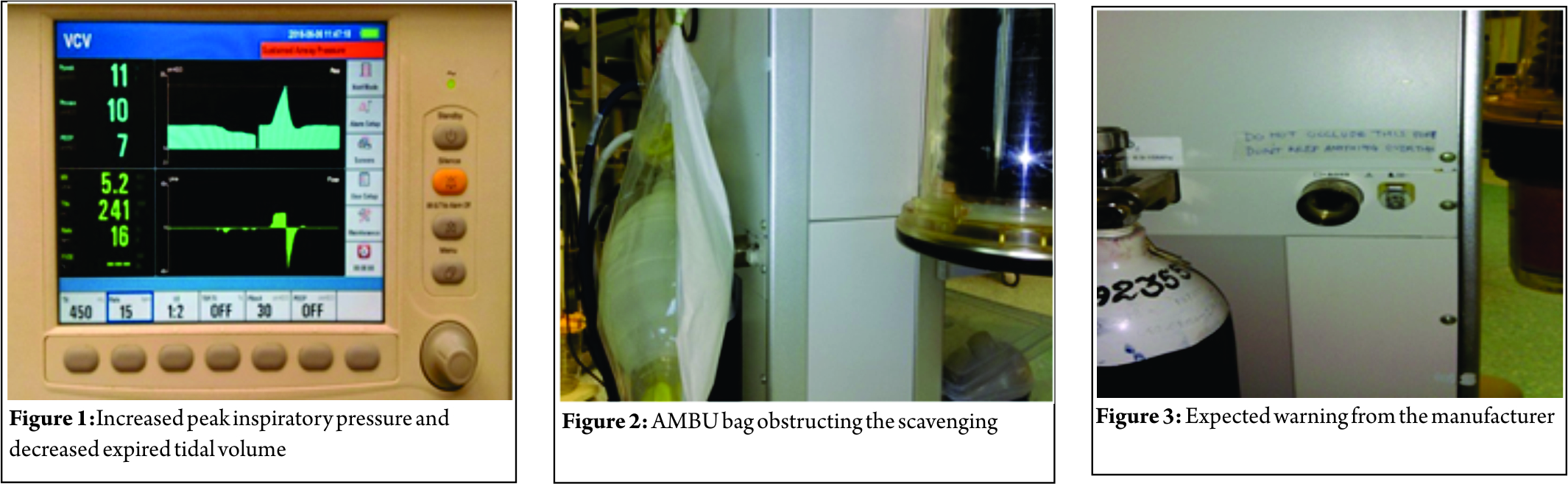
A 58 kg, a 70-year-old male patient with chronic obstructive pulmonary disease was scheduled for Koch’s spine vertebral D10 collapse and compression for decompression and fixation of D10–D12 vertebra in prone position. Anesthesia machine with circle system and anesthesia ventilator (Mindray WATO-EX35 anesthesia machine; Shenzhen Mindray Bio-medical Electronics Co. Ltd.) were checked as per standard institutional protocol. After adequate preoperative optimization of the patient, general anesthesia was induced with standard technique using midazolam, fentanyl, propofol, and vecuronium. After confirming endotracheal intubation, lungs were mechanically ventilated with tidal volume 450 ml, respiratory rate 14 per min, and inspiratory to expiratory ratio 1:2 without positive end-expiratory pressure (PEEP). The patient was made prone following the standard protocols on Wilson frame. While observing the peak airway pressure in ventilator display to adjust tidal volume, we noticed gradual increase in the baseline airway pressures which soon reached more than 10 cm of water with increasing peak inspiratory pressure and gradual decrease of expired tidal volume (Fig. 1). Severe reduction in tidal volume forced us to switch over to manual mode of ventilation with adjustable pressure limiting valve with which we were able to ventilate the patient with normal airway pressures. Meanwhile, the patient’s basic vital parameters were normal and there was no evidence of pneumothorax on auscultation. Manual ventilation was continued with stepwise approach to search for various causes of sustained airway pressures. Although no visible obstruction in the breathing circuit, heat and moisture exchanger (HME) filter, or endotracheal tube was observed, we immediately changed the breathing circuit and HME filter. One-way valves in the circle system were functioning properly. On auscultation of chest, breath sounds were heard equally on both the sides and clinically pneumothorax was ruled out. The soda lime CO2 absorber in the circle system was isolated to rule out any obstruction in this part of the circuit. Finally, we noticed a bag containing AMBU bag, which was hanged at the back of anesthesia machine was lying over the scavenging port outlet behind the machine (Fig. 2). Since our OT does not have either active or passive scavenging system, the transfer pipe for waste gas was missing, leaving the scavenging port open. The bag got stuck to the expiratory scavenging port causing almost complete obstruction. Removal of the bag at once resulted in immediate restoration of proper ventilation with airway pressures returning to normal levels. Stepwise troubleshooting of unexpected ventilatory problem in a systematic way averted major airway/ventilator catastrophe.
Conclusion
Critical incidents involving anesthesia breathing system can arise secondary to either equipment misuse or equipment failure. Equipment failure refers to malfunctioning of a device unexpectedly, despite regular maintenance and previous uneventful use [6]. Disconnection of the breathing system assembly has been found to be the most frequent cause of breathing system malfunction [7]. Obstruction of the breathing circuit is rapidly injurious the rapidity of event is usually attributed to the development of high intrathoracic pressure and thus producing PEEP-like effect causing reduction in venous return and leading on to the right ventricular filling volume and finally cardiac output [8]. Hence, to avoid such hazards, apart from routine standard anesthesia machine checkup, there should have been clear warning instructions written at the scavenging port outlet (Fig. 3) which was lacking in our anesthesia machine. A standard scavenging system consisting of a collecting assembly, transfer tubing, receiving system, and disposal system for waste gases is essential part of safe anesthesia delivery systems and should never be neglected. Another safeguard will be to incorporate some sort of sensor and audiovisual alarm for early detection of obstruction to the scavenging port outlet. Although there is no substitute for eternal vigilance of anesthesiologist taking care and managing the patient under anesthesia, systematic checking of anesthesia delivery systems and these modifications will provide additional margin of safety.
References
- Nunn G. Hazards of scavenging devices. Anaesthesia 1996;51:404-5.
- Khorasani A, Saatee S, Khader RD, Nasr NF. Inadvertent misconnection of the scavenger hose: A cause for increased pressure in the breathing circuit. Anesthesiology 2000;92:1501-2.
- Carvalho B. Hidden hazards of scavenging. Br J Anaesth 1999;83:532-3.
- Hamilton RC, Byrne J. Another cause of gas-scavenging-line obstruction. Anesthesiology 1979;51:365-6.
- Farquhar-Thomson DR, Goddard JM. The hazards of anaesthetic gas
scavenging systems. Anaesthesia 1996;51:860-2. - Raajesh J. Indo Iranian J Sci Res 2014;3.
- Satya-Krishna R. Complications in Anesthesia. 2nd ed. Philadelphia: Saunders; 2006. p. 527.
- Cairo JM, Pilbeam SP. Effects of positive pressure ventilation on the cardiovascular, cerebral, renal and other organ systems. In: Mechanical Ventilation Physiological and Clinical Application. 4th ed. Philadelphia: Mosby; 2006. p. 346-47.
| How to Cite this Article: Madankar D, Mathankar N. Scavenging Port Obstruction: A Case of Spinal Surgery in Prone Position. Journal of Anaesthesia and Critical Care Case Reports Jan-April 2018; 4(1):38-39. |
