Vol 9 | Issue 1 | January-April 2023 | Page: 09-12 | Suresh Jaganathan, Balaji Thirugnanam, Shanmugapriya Senthilkumar, Duraiyarassu Uthaman
DOI: https://doi.org/10.13107/jaccr.2023.v09i01.212
Author: Suresh Jaganathan [1], Balaji Thirugnanam [1], Shanmugapriya Senthilkumar [1], Duraiyarassu Uthaman [1]
[1] Department of Anaesthesiology and Critical Care, Preethi Hospitals, Madurai, Tamil Nadu, India.
Address of Correspondence
Dr. Suresh Jaganathan,
Department of Anaesthesiology and Critical Care, Preethi Hospitals, Madurai, Tamil Nadu, India.
E-mail: dr.lakshmi.naveen@gmail.com
Abstract
Blast injuries are rare, but life-threatening medical emergencies. A blast injury is a complex type of physical trauma resulting from direct or indirect exposure to an explosion. Blast is a process where any substance or device, capable of creating a sudden gas expansion, releasing potential energy and thus creating a pressure wave damaging the surrounding objects. Blast injury is becoming more common in non-military population due to terrorist acts and unsafe use of explosive equipment and substances, but it is still rare to see such injuries and deaths. Accidental blasts normally occur at work place which results from the handling of potentially hazardous equipment by untrained, unlicensed individuals or by the use of faulty, under -maintained equipment. The interpretation of blast injuries carries great importance in understanding the mechanism of these injuries, to correlate the clinical findings with the circumstances of the case and also help in the management of blast victims. We hereby describe a case of country bomb blast injury in a stone quarry where explosive device will be used to break stones. The purpose of this reported case is to highlight the clinical presentation of blast injury and possible clinical outcomes.
Keywords: Blast injury, Poly trauma , Amputation, Embolism.
Introduction
Explosions through an accident or intentional act are an occurrence that can cause serious injury and death. Injuries will be inflicted on many people at the same time resulting in high level of mortality and morbidity. The main mechanism causing the extent of injuries is the amount of kinetic energy released in a short time due to explosion . Management of survivors of blast injury is complex and time-consuming during the initial resuscitation in emergency department because of involvement of multiple surgical specialties and extensive radiographic imaging.
Case Presentation
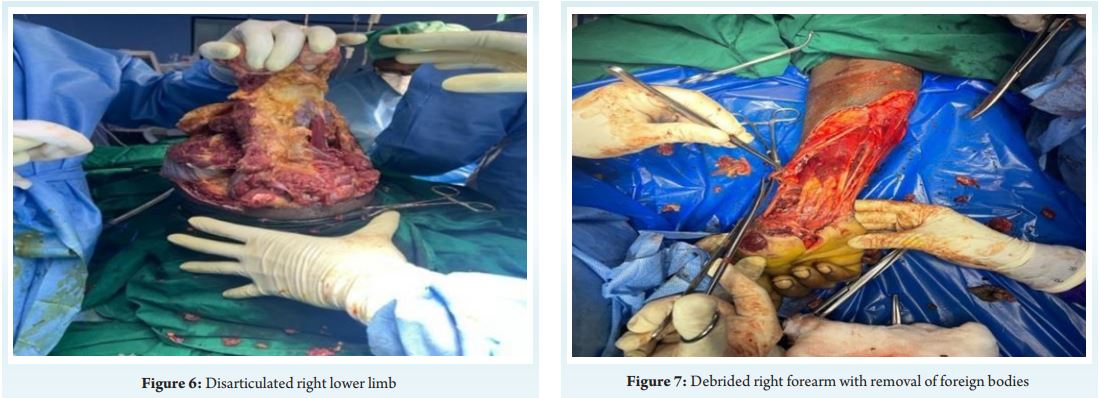
A 34-year-old male, quarry stone breaker by occupation sustained blast injury at his work spot in the morning. On arrival to emergency room he was drowsy, disoriented, pale with a pulse rate of 142/min and blood pressure of 72/40 mmHg. He was tachypneic with room air saturation of 97%. Primary survey revealed multiple foreign bodies (stone fragments) impacted over face, left arm, and right knee. He had traumatic amputation of right lower limb at the level of proximal tibia, open grade III B displaced comminuted both bone legs left leg with multiple irregular lacerations of left thigh and leg, multiple laceration of right forearm, penile degloving injury and laceration of left arm with brachial artery cut injury. He was resuscitated with crystalloids, colloids and blood products .Nor-adrenaline infusion was initiated at the rate of 0.3 mic/kg/min to maintain mean arterial pressure around 60 mmHg, Analgesics and tetanus prophylaxis were given. Necessary blood investigations and computerized tomography of brain, facial bones, thorax, abdomen and pelvis was done. After initial stabilization detailed secondary survey was done Computerized tomography scan of brain and facio maxillary region showed mild cerebral edema with effacement of ventricular system and sulci. Multiple hyperdense foreign bodies were noticed in scalp, perinasal, periorbital, pre maxillary and pre oral subcutaneous region. CT scan of thorax, abdomen and pelvis was found to be normal. In the operating room he was induced with ketamine 40 mg and etomidate 10 mg and intubated with 7.5 mm ID cuffed endotracheal tube under rapid sequence technique. Post intubation right internal jugular vein and left femoral artery was cannulated under ultrasound guidance. Anesthesia was maintained with air: oxygen mixture with sevoflurane as inhalational agent with volume controlled ventilation. Nor-adrenaline infusion was continued at the rate of 0.4 mic/kg/min during the intra operative period to titrate blood pressure. Serial blood gases done for correction of acidosis. He underwent wound debridement and removal of impacted foreign bodies, through knee disarticulation of right lower limb along with AO external fixator application of left tibia and brachial artery repair of left upper limb with cephalic vein graft and fasciotomy of left forearm under general anaesthesia. Standard monitoring with ECG, NIBP, invasive blood pressure, pulse oximeter, ETCO , end tidal volatile anaesthetic 2analyser and temperature monitoring was done. Post induction urinary catheter and ryles tube was inserted. Duration of surgery lasted approximately four hours. Postoperatively he was electively ventilated in view of hemodynamic instability and extubated the next day. A total of four packed red blood cell units, 6 fresh frozen plasma units were transfused during the intra operative period He further underwent two more wound debridement procedure in a staged manner and split skin graft later. He was discharged on 30 day after admission.


Discussion
Blunt and penetrating mechanism can cause classic injury patterns to several organ system from explosion [1]. Blast injury refers to the biophysical and pathophysiological events and the clinical syndrome and patho-anatomical changes caused by exposure of a living body to the shock wave generated by a detonated explosive [2]. The trauma team should manage bomb blast victims using systematic approach such as advanced trauma life support. Several injuries caused by blast wave may not apparent initially during triage. Bomb blast victims tend to be more severely injured and take up more resources. Differential pressure forces and eventual shearing at the tissue interface occurs when blast/ shock wave encounter tissue at different densities [3]. Four patterns of injuries had been described according to the mode of injury [4]. A fifth blast injury mechanism proposed recently as patient’s hyper inflammatory response is unrelated to severity of injury and complexity [ 5].Primary blast injuries can be subtle and have a deranged presentation . Blast lung should be considered in any victim who had dyspnea, cough, and hemoptysis. If the pressure exceeds 40 psi the victim can have pulmonary contusion, pneumothorax, air embolism, parenchymal damage or subcutaneous emphysema. The most common respiratory system injury is pulmonary contusion and its presentation can be delayed upto 48 hours. Blast ear should be considered in any victim who had hearing loss, tinnitus or bleeding from ear. When the ears are pressurized beyond 5 psi bony ossicles of ear can be dislocated ,fractured or permanently destroyed [6]. Blast eye should be considered in victims with eye pain, swelling or ecchymosis around orbit, bleeding from eye or blindness [7]. Pneumoperitoneum is a relatively rare complication of GI barotraumas. The colon is the most common site of hemorrhage and perforation [8]. The most common solid organ lesions reported were subcapsular hematoma in the liver, spleen, and kidneys [9]. Bomb fragments and debris released by intense energy of explosion causes secondary blast injury. These fragments are known as shrapnel. Penetrating and blunt trauma caused by these flying projectiles depends upon the size and speed of those projectiles. Secondary blast injuries are much more common than primary blast injuries. It is the most common cause of death in blast victims upto 10% of blast survivors have significant eye injuries [10].Propulsion of the victim’s body into another object by blast wind can result in such tertiary blast injuries. These effects result from bulk flow of gas away from explosion. A person who is flung into a fortified immovable object with velocity greater than 26 feet/second has a mortality rate of about 50% [11]. Fractures and head injuries are the most common. This category of quaternary blast injuries includes burns from fire or radiation, crush injuries, associated with structural collapse, poisoning from carbon monoxide or other toxic products of explosion and chemical or dust inhalation. Carboxy haemoglobin should be obtained in patients who have been exposed to blast in an enclosed area. Immediate death may occur from massive pulmonary bleeding with rapid suffocation despite effective care. Massive air embolism or significant brain injury or traumatic amputation can cause immediate death. Acute air embolism may be the most common cause of rapid death in initial survivor of blast when positive pressure ventilation is initiated [12].Usually the severely injured will arrive after the less injured patients in emergency room. The less injured often skip emergency service and proceed directly to the closest hospitals. For a rough prediction of the number of first wave of casualties, double the first hour’s casualty count. The injury pattern seen after a detonation of an explosive are blunt, thermal and penetrating trauma are usually known to pre hospital providers, emergency physicians, and orthopaedic surgeons [13]. After a thorough physical examination the physician should look for sentinel signs of potentially significant blast exposure. The most important step of management is assessment of life support needs and ensuring that the patient has an adequate airway, appropriate ventilation, and adequate circulation. The only laboratory study that is useful is serial hemoglobin determinations. Chest X-ray should be done in all patients who near a significant explosion. Computerized tomography of brain, chest, abdomen, pelvis should be done if there is pathology in these areas.
Conclusion
The evaluation of a patient with blast injuries depends on the nature of explosion and fragments produced, distance of victim from explosion, and fragments. Management of bomb blast injuries is very challenging since blast victims show a combination of blast, blunt, penetrating and thermal trauma which increases morbidity and mortality. Burn injured patients who can be managed in burn centers must be cleared of potential traumatic injuries.
Clinical message
Bomb blast injuries are medical emergencies. Traumatic amputation of limbs caused by bomb blast carries a high risk of mortality. The severity of blast injuries varies in relation to the power and quantity of the explosive, open or confined space, and the proximity of the victim to the center of explosion. Given these characteristics, it is important to have a classification that highlights the groupings of all the documented injuries as primary to direct them towards a correlation with the scene and center of explosion. The entire trauma team should work in a well coordinate manner following advanced life support protocol to treat bomb blast casualties effectively and efficiently.
References
1. David L Ciraulo , Eric R Frykberg, David V Feliciano, Thomas E Knuth, Charles M Richart, Christy D Westmoreland, Kathryn A Williams. A survey assessment of the level of preparedness for domestic terrorism and mass casualty incidents among Eastern Association for the Surgery of Trauma members J Trauma 2004 May;56(5):1033-9
2. Explosions and blast injuries: A primer for clinicians. Centers for Disease Control and Prevention web site www.cdc.gov/masstrauma/preparedness/primer.pdf. Accessed 1/21
3. Wightman JM, Wayne BA. Blast and crush injuries. In: Tintinalli JE, Kelen GD, Stapczynski JS, editors. Emergency Medicine-A Comprehensive Study Guide. 6th ed. New York: McGraw- Hill; 2004. pp. 46–50. [Google Scholar]/04.
4. Stephen J Wolf 1 , Vikhyat S Bebarta, Carl J Bonnett, Peter T Pons, Stephen V Cantrill. Blast injuries Lancet 2009 Aug 1;374(9687):405-15
5. Sorkin P, Nimrod A, Biderman P, et al. The quinary (Vth) injury pattern of blast. J Trauma. 2004;56:232. [Mil Med
6. Steven T Williams 1 , Thomas H Harding 1 , J Keegan Statz 1 , John S Martin. Blast Wave Dynamics at the Cornea as a Function of Eye Protection Form and Fit 2017 Mar;182(S1):226-229. Google Scholar
7. Ajay K Singh ,Noah G Ditkofsky, John D York , Hani H Abujudeh , Laura A Avery , John F Brunner Aaron D Sodickson , Michael H Lev 1 Radiographics Jan-Feb 2016;36(1):295-307.
8. Huller T. Bazini Y. Blast injury of the chest and abdomen. Arch Surg 1970;100:24.
9. Argyros GJ. Management of primary blast injury. Toxicology 1997;121:105-115
10. Explosions and blast injuries: A primer for clinicians. Centers for Disease Control and Prevention web site www.cdc.gov/masstrauma/preparedness/primer.pdf. Accessed 1/21/04.
11. Stapczynski JS. Blast injuries. Ann Emerg Med 1982;11:687-694
12. Wightman JM, Gladish SL. Explosions and blast injuries. Ann Emerg Med. 2001;37:664– 78. [PubMed] [Google Scholar]
13. Weiner SL, Barrett J. Explosions and explosive device-related injuries. In: Trauma Management for Civilian and Military Physicians. Philadelphia; Saunders: 1986:13-26.
| How to Cite this Article: Jaganathan S, Thirugnanam B, Senthilkumar S, Uthaman D | Resuscitation and Management of Bomb Blast Survivor- A Challenge in Real | Journal of Anaesthesia and Critical Care Case Reports | January-April 2023; 9(1): 09-12 | https://doi.org/10.13107/jaccr.2023.v09i01.212 |