Vol 9 | Issue 2 | May-August 2023 | Page: 01-04 | Kazutomo Saito, Masanori Yamauchi
DOI: https://doi.org/10.13107/jaccr.2023.v09i02.215
Author: Kazutomo Saito, Masanori Yamauchi [1]
[1] Anaesthesiology and Perioperative Medicine, Tohoku University Graduate School of Medicine, 2-1 Seiryomachi, Aoba-ku, Sendai, Miyagi, Japan.
Address of Correspondence
Dr. Kazutomo Saito
Anaesthesiology and Perioperative Medicine, Tohoku University Graduate School of Medicine, 2-1 Seiryomachi, Aoba-ku, Sendai, Miyagi, Japan.
E-mail: kazutomo@med.tohoku.ac.jp
Abstract
Introduction: Papillary thyroid carcinoma with an extensive tumor thrombus growing into the superior vena cava and right atrium is rare. Only a few case reports have described the surgical resection of thyroid carcinoma and extensive tumor thrombus under cardiopulmonary bypass.
Case presentation: We encountered a 79-year-old woman with papillary thyroid carcinoma who developed severe superior vena cava syndrome caused by an extensive tumor thrombus. Radical resection of the thyroid carcinoma and tumor thrombus was performed under cardiopulmonary bypass. Both the innominate vein and inferior vena cava pressures were continuously monitored during the surgical procedure. The innominate vein pressure was measured using a peripherally inserted central venous catheter (PICC) via the left basilic vein. The initial central venous pressures at the innominate vein and inferior vena cava were 22 mmHg and 8 mmHg, respectively. After tumor resection, the pressure gradient between the innominate vein and inferior vena cava was markedly decreased. At the end of the surgery, the pressure gradient had almost disappeared.
Conclusion: Central venous pressure monitoring at the innominate vein through PICC was useful in detecting the failure of venous drainage from the innominate vein or in diagnosing the perioperative recurrence of superior vena cava syndrome due to innominate vein stenosis.
Keywords: Superior vena cava syndrome, Innominate vein pressure, Peripherally inserted central venous catheter
Introduction
Papillary thyroid carcinoma typically has a good prognosis and rarely shows extensive tumor thrombus growing into the superior vena cava (SVC) and right atrium [1]. The blocking of venous return associated with tumor thrombus causes superior vena cava syndrome (SVCS), impairs the quality of life, and is life-threatening [2]. The signs and symptoms of SVCS include edema in the upper body, excessive venous stasis, and development of collateral blood circulation accompanied by increased venous pressure. Tumor thrombus in the right atrium poses a high risk of sudden death due to pulmonary embolism [3]; therefore, radical resection of the thyroid cancer and extensive tumor thrombus should be considered. We encountered a 79-year-old woman with papillary thyroid carcinoma who developed severe SVCS caused by an extensive tumor thrombus that was successfully resected under cardiopulmonary bypass (CPB). Only a few case reports have described the surgical resection of thyroid carcinoma and extensive tumor thrombus under CPB support [4–6]. Continuous monitoring of both the innominate vein, measured through a peripherally inserted central venous catheter (PICC) inserted via the left basilic vein, and inferior vena cava (IVC) pressures during the surgical procedure is extremely rare.
Case Presentation
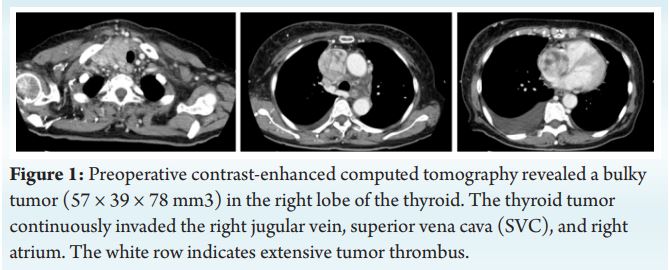
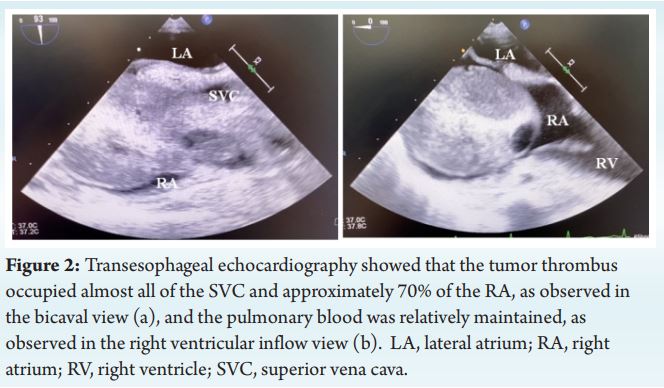
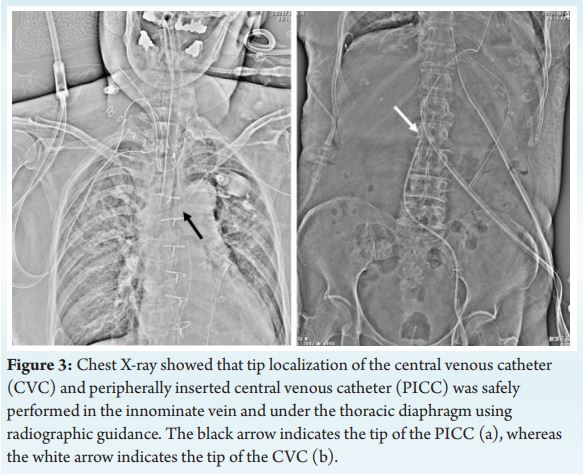
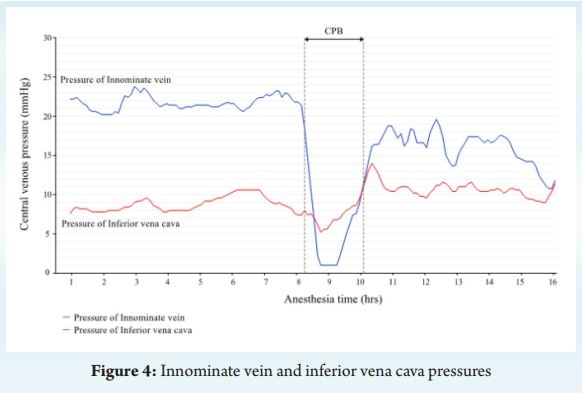
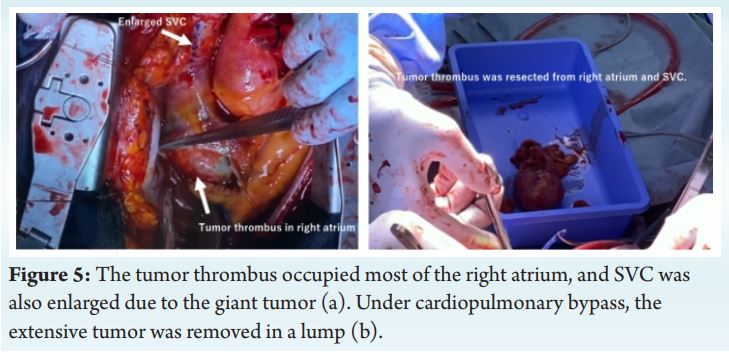
A 79-year-old woman had edema in the face and right upper limb for 1 year and was aware of a cervical mass for 6 months. Fine-needle aspiration biopsy of the neck mass confirmed a diagnosis of papillary thyroid carcinoma. Preoperative computed tomography (CT) 3revealed a bulky large tumor (57 × 39 × 78 mm ) in the right lobe of the thyroid, and the tumor thrombus extended continuously into the right jugular vein, the right side of innominate vein, SVC, and reaching up to the right atrium (Fig. 1). The peripheral vascular invasion was not obviously observed. Transthoracic echocardiography showed that the tumor thrombus occupied approximately 70% of the right atrium but did not invade the tricuspid valve. The trachea was displaced to the left; however, the patient did not complain of respiratory discomfort at rest, and hoarseness due to vocal cord paralysis was absent. Extensive venous collaterals developed because of severe SVCS. Thus, thyroidectomy and tumor thrombus removal under CPB were performed to eliminate the symptoms of SVCS. The intravenous tumor thrombus, if ruptured, could induce pulmonary embolism, which may lead to sudden death. Therefore, early resection of the tumor thrombus is desirable. If the tumor thrombus unfortunately ruptures intraoperatively, the hemodynamic status will become unstable, and CPB support may be required in the worst scenario. Although upper gastrointestinal endoscopy detected esophageal varices with a red color sign, we decided to monitor the motion of the tumor thrombus in the right atrium using transesophageal echocardiography (TEE) to prevent pulmonary embolism. Moreover, regional cerebral oxygen saturation (rSO ) at 2the right and left foreheads (INVOS™ 5100 C, Somanetics, USA) was initiated prior to the administration of general anesthesia, and both the innominate vein and the IVC pressures were continuously measured to prevent brain edema. The innominate vein pressure was measured through PICC (PowerPICC®, Medicon, Japan) which was inserted via the left basilic vein. On the other hand, the IVC pressure was measured through a central venous catheter (CVC) (SMAC™ Plus, Covidien, Japan) which was inserted via the left femoral vein.After administration of 100% oxygen, general anaesthesia was induced by continuous infusion of 0.25 μg/kg/min of remifentanil as well as intravenous bolus administration of 60 mg of propofol, 0.15 mg of fentanyl, and 50 mg of rocuronium. She was intubated using an electromyographic endotracheal tube (TriVantage®, Medtronic, Ireland). After tracheal intubation, the TEE probe was inserted. TEE showed that the tumor thrombus occupied almost all of the SVC and approximately 70% of the right atrium, as observed in the bicaval view, and the pulmonary blood was relatively maintained, as observed in the right ventricular inflow view (Fig. 2). General anaesthesia was maintained by continuous infusion of propofol (4–5 mg/kg/h) and remifentanil (0.1–0.3 μg/kg/min). Administration of rocuronium was limited to anaesthesia induction and CPB because of intraoperative neuromonitoring during thyroidectomy. Systemic arterial pressure was measured via the right radial artery, and the peripheral venous infusion line was inserted in the lower limb. Subsequently, a central venous catheter (CVC) (SMAC™ Plus, Covidien, Japan) was inserted via the left femoral vein. Additionally, a peripherally inserted central venous catheter (PICC) (PowerPICC®, Medicon, Japan) was inserted via the left basilic vein. Tip localization of the PICC and CVC was safely performed in the innominate vein and under the thoracic diaphragm using radiographic guidance to avoid interference with the tumor thrombus (Fig. 3).During the surgical procedure, the systemic arterial pressure, central venous pressure (CVP) at the innominate vein and IVC, and rSO2were continuously monitored. The initial CVPs at the innominate vein and IVC were 22 mmHg and 8 mmHg, respectively (normal range, 2–8 mmHg) (Fig. 4).Under general anaesthesia, standard median sternotomy was performed after adhesiolysis of the cervical thyroid tumor. The innominate vein, SVC, and right subclavian vein were exposed. The cardiac surgeons macroscopically confirmed that the tumor thrombus in the SVC obstructed the blood flow in the innominate vein, causing remarkable enlargement of the innominate vein. The innominate vein and IVC were used for venous drainage, and antegrade systemic perfusion was performed via the ascending aorta. The blood lost from the right atrium was retrieved using a suction system. For anticoagulation, heparin was administered at 15,000 U (0.3 U/kg), and activated clotting time was controlled above 450s during CPB. This was performed with the heart beating using a pump. The tumor thrombus in right atrium, SVC, and innominate vein was removed (Fig. 5). Because the tumor thrombus did not invade the venous wall, SVC reconstruction was not performed. During the detachment of the tumor thrombus, a part of the SVC wall was injured; therefore, this was repaired using autologous pericardium. CPB weaning was uneventful and completed without catecholamine support. To reduce the CPB time as much as possible, a right jugular venotomy was performed after CPB, and the tumor thrombus in the right jugular vein and the thyroid tumor were subsequently removed. During tumor resection, the right jugular venous wall was damaged, resulting in a major hemorrhage. The patient required massive transfusion support (9,520 mL of concentrated red blood cells, 9,600 mL of fresh-frozen plasma, 1,000 mL of platelet concentrates, and six units of cryoprecipitate) for severe intraoperative bleeding. The total volume of blood loss was 10,889 mL. For the rapid infusion device, we used Belmont® Rapid Infuser (Mediconovus, Japan) connected to the introducer sheath via the left femoral vein. A massive hemorrhage occurred, lasting for approximately 4 hour. The amount of blood loss per hour reached approximately 2,000 mL. However, by transfusion of adequate blood components, her hemodynamic status was relatively stabilized. CPB, surgery, and anaesthesia lasted for 1 hour 47 minutes, 13 hour 34 minutes, and 16 hour 10 minutes, respectively. At baseline, the CVPs at the innominate vein and IVC were 22 mmHg and 8 mmHg, respectively. After tumor removal, the pressure gradient decreased from 17 mmHg to 11 mmHg. Although the pressure gradient remained during hemostasis, it nearly disappeared at the end of the operation (Fig. 4). The bilateral recurrent laryngeal nerves were protected using neuromonitoring with the electomyopgraphic endotracheal tube. Following the completion of surgery, the patient was transferred to the intensive care unit with ventilator support under propofol sedation. Fiberoptic laryngoscopy on postoperative day (POD) 1 revealed edema of the piriform recess and arytenoid cartilage. After improvement of laryngeal edema, the patient was weaned from mechanical ventilation on POD 4. After extubation of the tracheal tube, her consciousness level was clear, and she did not complain of hoarseness.
Discussion
Papilloma thyroid carcinoma is commonly considered to be of low risk and rarely invades the jugular vein, SVC, and right atrium. Extrathyroidal intravascular invasion occurs in only 1.3% of this patient group [1]. A few case reports, including the current one, have described the resection of a thyroid tumor with extensive tumor thrombus growing into the right atrium under CPB [4–7]. Continuous monitoring of the innominate vein pressure via a PICC and the IVC pressure via a CVC during surgical procedures had not been reported except in the present case. In the present case, severe SVCS was induced by a giant tumor thrombus; thus, radical resection of the papillary thyroid tumor and tumor thrombus was performed under CPB.CPB is commonly established with separate cannulation of the SVC, IVC, and ascending aorta. Poor venous drainage through the SVC can induce brain edema. To protect the central nervous system during CPB, the SVC pressure is routinely monitored during cardiac surgery. However, in this case, the right jugular vein was occupied by the tumor thrombus, the left jugular vein was included in the surgical field, and insertion of a CVC via bilateral jugular veins was impossible. Therefore, we implanted a PICC in the left basilic vein. The tip of the PICC was placed on the left side of the innominate vein by radiographic guidance to avoid interference with the tumor thrombus, and the drainage cannula was inserted into the innominate vein.In this case, the CVC and PICC were inserted via the left femoral vein and left basilic vein, respectively, and the pressure gradient between the innominate vein and IVC was continuously monitored. In this case, the placement of PICC was important because CVP monitoring at the innominate vein was useful in detecting the failure of venous drainage from the innominate vein or in diagnosing the postoperative recurrence of SVCS due to innominate vein stenosis. Moreover, the PICC is helpful in postoperative infusion therapy. If the CVC cannot be inserted via the bilateral jugular vein because of tumor thrombus or surgical field, PICC insertion via the basilic vein should be considered.
Conclusion
We present a case of resection of papillary thyroid carcinoma occupying the right jugular vein, SVC, and right atrium under CPB in a patient with severe SVCS. If the CVC cannot be inserted via the bilateral jugular vein because of a giant thyroid tumor or surgical field, PICC insertion via the basilic vein should be considered. CVP monitoring at the innominate vein is also beneficial for detecting the failure of venous drainage from the innominate vein or for diagnosing the perioperative recurrence of SVCS due to innominate vein stenosis.
Clinical Message
• We encountered a 79-year-old woman with papillary thyroid carcinoma who developed severe superior vena cava syndrome caused by an extensive tumor thrombus.
• Only a few case reports have described the surgical resection of thyroid carcinoma and extensive tumor thrombus under cardiopulmonary bypass.
• Continuous monitoring of both the innominate vein and inferior vena cava pressures during the surgical procedure is extremely rare.
• Central venous pressure monitoring at the innominate vein was useful in detecting the failure of venous drainage from the innominate vein or in diagnosing the perioperative recurrence of severe superior vena cava syndrome due to innominate vein stenosis.
References
[1] Kowalski LP, Filho JG. Results of the treatment of locally invasive thyroid carcinoma. Head Neck 2002;24:340–4.
[2] Wilson LD, Detterbeck FC, Yahalom J. Clinical practice. Superior vena cava syndrome with malignant causes. N Engl J Med 2007;356:1862–9.
[3] Ordookhani A, Motazedi A, Burman KD. Thrombosis in thyroid cancer. Int J Endocrinol Metab 2017;16:e57897.
[4] Hasegawa S, Otake Y, Bando T, Cho H, Inui K, Wada H. Pulmonary dissemination of tumor cells after extended resection of thyroid carcinoma with cardiopulmonary bypass. J Thorac Cardiovasc Surg 2002;124:635–6.
[5] Yamagami Y, Tori M, Sakaki M, Ohtake S, Nakahara M, Nakao K. Thyroid carcinoma with extensive tumor thrombus in the atrium. Gen Thorac Cardiovasc Surg 2008;56:555–8.
[6] Chen W, Lei J, Wang Y, et al. Case report: superior vena cava resection and reconstruction for invasive thyroid cancer: report of three cases and literature review. Front Surg 2021;8:644605.
[7] Chen H, Ng V, Kane CJ, Russell IA. The role of transesophageal echocardiography in rapid diagnosis and treatment of migratory tumor embolus. Anesth Analg 2004;99:357–9.
| How to Cite this Article: Saito K, Yamauchi M | Resection of Papillary Thyroid Carcinoma Occupying the Superior Vena Cava and Right Atrium under Cardiopulmonary Bypass in a Patient with Severe Superior Vena Cava Syndrome: A Case Report | Journal of Anaesthesia and Critical Care Case Reports | May-August 2023; 9(2): 01-04. https://doi.org/10.13107/jaccr.2023.v09i02.215 |