Vol 1 | Issue 1 | July – Sep 2015 | page:12-15 | Priyanka Sunil Shalu[1], Poonam S Ghodki.
Authors: Priyanka Sunil Shalu[1], Poonam S Ghodki [2].
[1] Maharashtra University Of Health Science.
[2] Shrimati Kashibai, Navale Medical College and General Hospital, Pune, India.
Address of Correspondence
Dr .Priyanka Sunil Shalu 3B/16 Aditya garden city phase 1 warje pune. State maharashtra. India. Pin 411058
Email: vikram146@gmail.com
Abstract
Introduction: Systemic sclerosis (SSc) also termed as scleroderma is a progressive autoimmune disease characterised by excessive accumulation of connective tissue components and vascular abnormalities, having variable presentation. Although many patients have a long survival rate, minority of them may progress to death due to visceral involvement in which renal involvement is the most common cause of mortality. The disease being a multisystem disorder has specific anaesthetic considerations. In this article, we report a rare case of progressive systemic sclerosis posted for vaginal hysterectomy which was performed successfully under spinal anaesthesia.
Keywords: Systemic sclerosis, Anaesthesia.
Introduction
Systemic sclerosis is a disorder of unknown aetiology involving multiple systems. It’s incidence is 2.3 to 10 per million in the adult population. 1,2 The disease process has the characteristics of both collagen vascular and an autoimmune disease with typical onset during 20-40 years of life, more commonly affecting females. 3 In some patients disease evolves into CREST syndrome (calcinosis, Raynaud’s phenomenon, esophageal hypomotility, sclerodactyly, telangiectasia). 3 Visceral involvement results in poor prognosis of the disease.4 We present a rare patient with systemic sclerosis undergoing vaginal hysterectomy. The features of systemic sclerosis with anaesthetic implications have been described.
Case report
A 33 year old female patient, with height 152 cm and weighing 58 kg with history of systemic sclerosis came to our hospital complaining of uterine prolapse. She had generalised body weakness and joint pain since long. She also complained of dry cough on and off which was associated with chest pain. Since two years she had progressive difficulty in swallowing solid food accompanied with heart burn and frequent regurgitation. Two years back she presented to a dermatological clinic with history of dryness of skin, sensitivity to cold of the digits suggestive of Raynaud’s phenomenon, difficulty in mouth opening and itching all over the body. After all investigations and skin punch biopsy she was diagnosed as a case of systemic sclerosis. She was also evaluated for autoantibodies that turned out to be anti-Scl-70 positive. Hypertension was detected at an early age of 31 years and was treated with Tab Amlodipine 5 mg. and Tab Enalapril 5mg once a day.
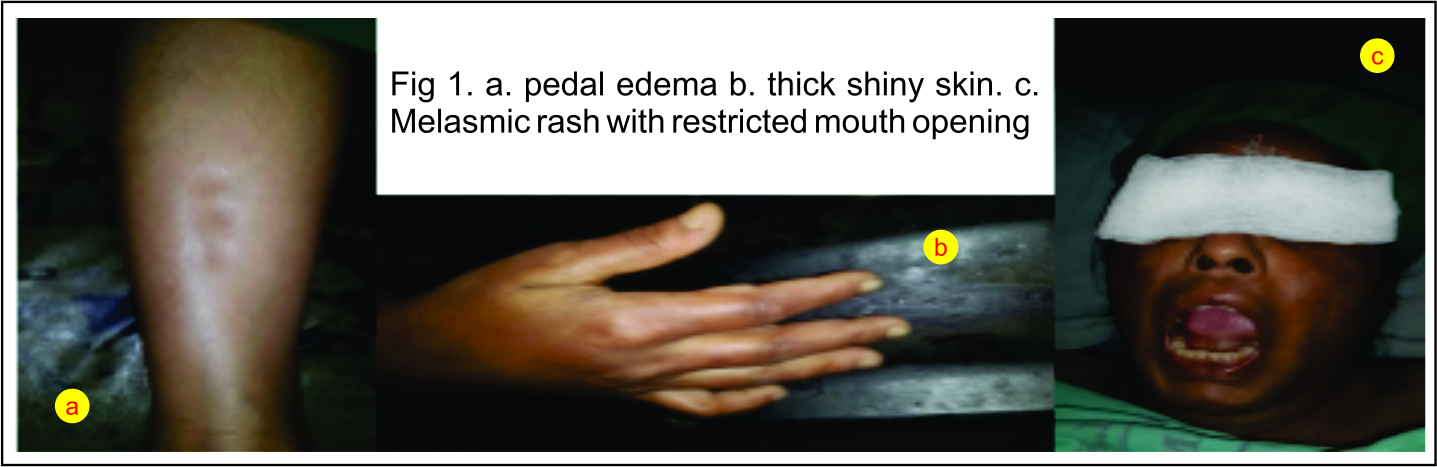
On physical examination she had waxy, smooth, thick and shiny skin (Fig 1b), decreased mouth opening of about two and half fingers (Fig 1c) with thyromental distance of 6 cm. On cutaneous examination, hyper pigmented melasmic patches were seen on face (Fig 1c). Skin was tightly adherent to underlying cutis. Non pitting edema (fig 1a) was detected on both lower limbs. She had decreased breath sound all over chest. On cardiovascular examination, her pulse rate and blood pressure were 92 beats per minute and 140/90 mmHg respectively. Rest of the systemic examination was within normal limits.
On admission, her haemoglobin was 12.4 gm/dL with normal platelet count and total and differential leucocyte count. Coagulation screening was normal. Her ESR was slightly elevated. Renal and liver function tests were normal. On urine examination, proteinuria (4+) was found. 2D echo findings were within normal limits.
She was investigated for her chest and gastrointestinal complaints; chest radiograph showed few reticular opacities in both basal zones. CT thorax showed changes of pulmonary fibrosis. She was further investigated with pulmonary function tests and arterial blood gas analysis. On pulmonary function tests there was mild restriction and values of arterial blood gas analysis were within normal limits. For evaluation of dysphagia barium swallow was performed which showed dilated oesophagus with narrowing in distal part without any filling defect.
Regional anaesthesia was preferred in this patient in view of potential risk of difficult intubation and regurgitation. Therefore the patient was prepared for vaginal hysterectomy
under spinal anaesthesia. However everything was kept ready for general anaesthesia. The procedure was explained to the patient and 150mg ranitidine and 4mg ondansetron was administered two hours preoperatively.
The patient was shifted to pre-warmed operation theatre, in view of history of Raynaud’s phenomenon. On arrival in OT her non-invasive blood pressure was 148/92 mm Hg and heart rate was 96 beats per minutes. On air O2 saturation was 96%. 20 gauge vein flow catheter was accessed with difficulty on dorsum of left hand and 500ml ringers lactate solution was infused over 20 minutes. Continuous ECG (lead II), heart rate, non-invasive blood pressure, pulse oximetry monitoring were used throughout the procedure. Pulse oximetry probe was frequently changed and applied at different
digits. Injection phenylephrine was kept ready.
The patient was placed in sitting position with 26 gauge Quincke’s spinal needle subarachnoid space was located at L2-L3 level with free flow of cerebrospinal flow. Hyperbaric bupivacaine 0.5% 17.5 mg was injected over 30 seconds. Immediately after injection patient was kept in supine position. Sensory block was evaluated by pin prick test and motor block was evaluated by modified Bromage scale. Ten minutes after the injection of drug, sensory block was reached at T8 dermatome and Bromage scale was 3.
After 15 minutes of block, lithotomy position was given. Temperature of OT was maintained at 24°C to avoid vasospasm.
Estimated blood loss during surgery was minimal (about 200ml) and total fluid given
during surgery was 2000ml (1500 ml of ringers lactate and 500 ml of DNS). There was no remarkable variation in hemodynamic and oxygen saturation value from baseline.
After spinal injection, motor block regressed at 180 minute and sensory block regressed at 250 min. Patient was monitored in post anaesthesia care unit for 24 hours and then shifted to gynaecology ward. On 5th day she was discharged from hospital uneventfully.
Discussion
Systemic sclerosis is a multisystem disorder of unknown aetiology. Disease can be thought of continuous process that spans varied clinical phenotypes from asymptomatic biological abnormalities to severe life threatening process.(1) Skin thickness progression rate is a measure of mortality and extent of visceral involvement. Prognosis is poor and is related to the extent of visceral involvement.(2,3) 50% survival rate is seen with limited cutaneous systemic sclerosis while survival rate with diffuse disease is as low as 25%.(2) Variable degree of extra cellular matrix accumulation (mainly collagen) occurs in both skin and viscera and is associated with specific autoantibodies most notably anticentromere and anti-Scl-70. (4) In our patient, anti-Scl antibodies were found. Familial occurrence of systemic sclerosis is quite rare and genetic associations are lacking. (4) Immune system is involved in initiation of fibrotic process and persistence occurs due to impaired regulation of collagen gene expression.(5)
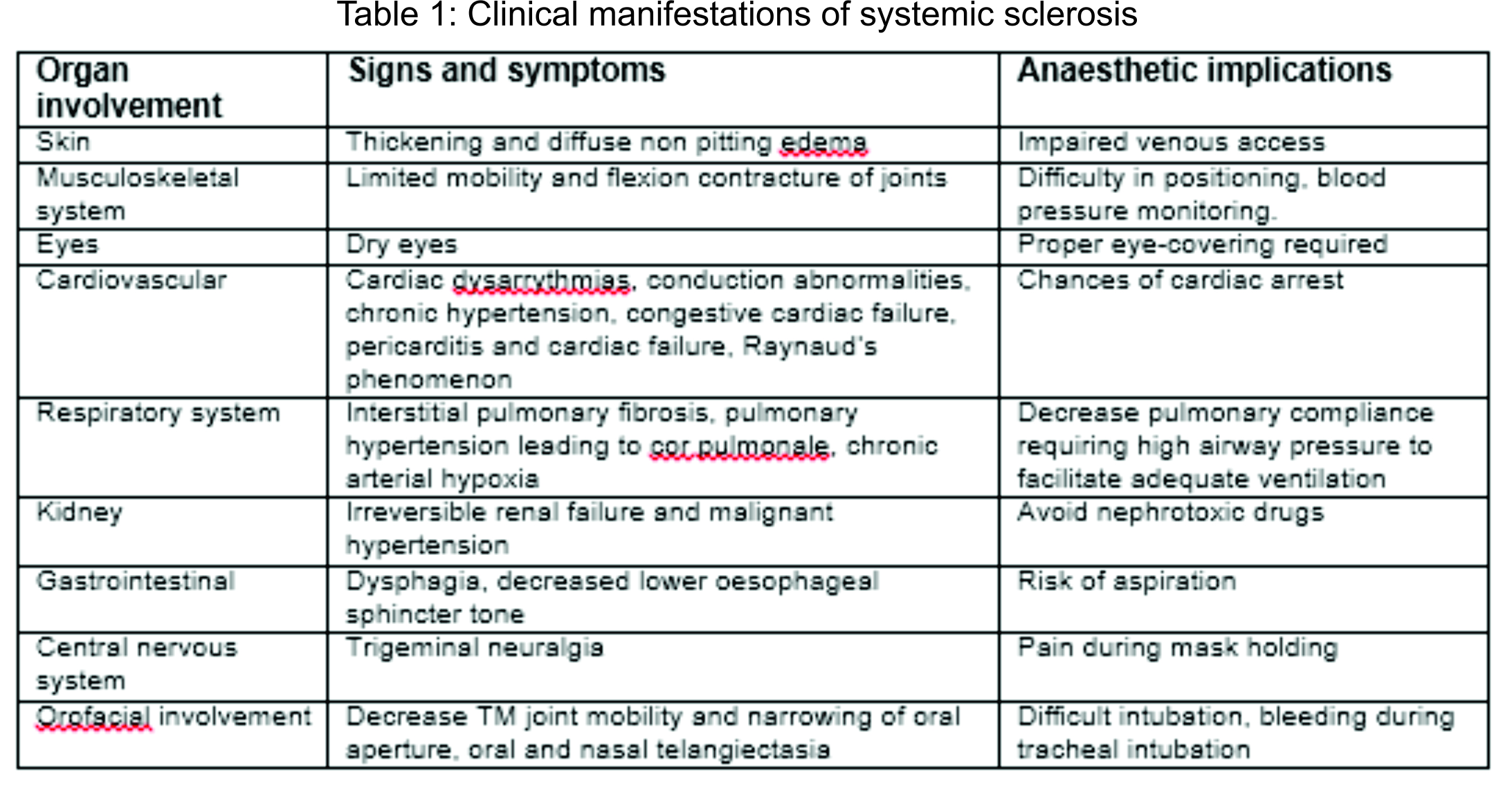
In general disease heterogeneity (stage, severity and pattern) is an important factor in therapeutic plan. Success with disease modifying therapy (cyclosporine, methotrexate and photophoresis) is modest and organ specific treatment e.g. ACE inhibitors for renal crisis can be dramatically successful. Interferon (alpha) having anti fibrotic effect can also be used.(5) Corticosteroids are avoided as they can precipitate renal crisis.(3) The clinical effects of excessive fibrosis and vascular damage which occur in systemic sclerosis have important implications for the anaesthetists, as explained in following table 1.
Renal disease is a major cause of mortality in systemic sclerosis. Histologically there is arteriolar intimal proliferation leading to decrease in renal blood flow. Variable presentations have been reported like chronic proteinuria, uraemia, systemic hypertension and rapidly progressive renal failure.(3, 10) Angiotensin converting enzyme inhibitors are the first line of treatment to control hypertension in renal systemic sclerosis and further progression of renal disease.(9, 11) Our patient had proteinuria (4+) and diagnosed as hypertensive which was treated with Tab Amlodipine and to prevent further renal damage Tab Enalapril was added.
Whenever possible regional anaesthesia is preferred technique in patients with systemic sclerosis to avoid risk of aspiration and failed intubation.(8,9) But regional anaesthesia should also be used cautiously to prevent risk of total spinal or inadequate anaesthesia which again requires tracheal intubation. In cases where general anaesthesia is the only choice, awake fibreoptic intubation is preferred especially when mouth opening is limited. It also preserves spontaneous respiration which is helpful if difficulty arises and also the cough reflex if regurgitation occurs. (7, 11) Rapid sequence induction should be avoided, in spite of the high risk of aspiration, due to the risk of difficult intubation. Moreover Sellick’s manoeuvre may be ineffective due to fibrosis of the oesophagus. (12, 13) In particularly difficult situations, it may be necessary to consider awake tracheostomy with local anaesthesia. (14, 15)
When the available literature was reviewed, we found that smaller dose of local anaesthesia is required as systemic sclerosis exhibits prolonged sensory and motor blockade. (9) This may be due to fibrosis of muscles, connective tissue, fascial planes surrounding to peripheral nerves are relatively inelastic which may lead to rise in compartment pressure on injection of local anaesthetic agent. (16, 17) However in our case we used routine dose of local anaesthetic (Hyperbaric bupivacaine 0.5% 17.5 mg) without any complication.
As vasoconstriction is a feature of systemic sclerosis, patient usually has contracted intravascular volume. This may manifest as refractory hypotension during and after induction of anaesthesia. These patients are often unresponsive to vasopressors which may worsen vasoconstriction in upper limbs. (3,15) Hence adequate preloading is important in these patients, but care should be taken to avoid rebound pulmonary edema on resolution of neuraxial block and return of intravascular tone. To avoid these complications combined spinal epidural technique may be used which allows dense and low block with intrathecal injection and anaesthesia can be gradually completed using epidural block. (18,19)
General care that should be taken during anaesthesia in systemic sclerosis patient includes careful positioning, padding to avoid pressure necrosis, wrapping of limbs for protection from cold, use of warm operation theatre and warm intravenous fluid, proper padding of eyes. Non-invasive blood pressure monitoring is preferred over arterial cannulation, prolonged application of pulse oximeter one digit should be avoided. In case of difficult venous access central venous catheterisation may be preferred. In our patient, despite of severe scleroderma, we were successful in gaining intravenous access, but that may not be possible always.
Conclusion
In conclusion we have described successful use of spinal anaesthesia for vaginal hysterectomy in a patient with systemic sclerosis. Careful pre-operative assessment is required to know the systemic involvement and determine the plan of anaesthesia. Such patients should be thoroughly investigated before planning anaesthesia.
References
1. LeRoy EC, Black CM, Fleischmajer R et al Scleroderma (systemic sclerosis): classification, subsets and pathogenesis. Journal of Rheumatology 1988; 15: 202–5.PubMed,CAS,Web of Science® Times Cited: 1364.
2. Giordano M, Valentini G, Migliaresi S, Picillo U, Vatti M. Different antibody patterns and different prognoses in patients with scleroderma with various extent of skin sclerosis. Journal of Rheumatology 1986; 13: 911–16.PubMed,CAS,Web of Science® Times Cited: 142.
3. Stoelting’s anaesthesia and coesixting disease 5th edition, page 486-487
4. Briggs DC, Black CM, Welsh KI. Genetic factors in scleroderma. Rheumatic Disease Clinics of North America 1990; 16: 31–51.PubMed,CAS,Web of Science® Times Cited: 36.
5. Report of a meeting of physicians and scientists, Royal Free Hospital School of Medicine London. Lancet 1996; 347: 1453–8.PubMed,Web of Science® Times Cited: 35.
6. Younker D & Harrison B. Scleroderma and pregnancy: anaesthetic considerations. British Journal of Anaesthesia 1985; 57: 1136–CrossRef,PubMed,CAS,Web of Science® Times Cited: 16.
7. HseuSS, Sung CS, Mao CC, Tsai SK, Lee TK. Anesthetic management in a parturient with progressive systemic sclerosis during Cesarean section — a case report. ActaAnaesthesiologica Singapore 1997; 35: 161–7 PubMed,CAS.
8. D’Angelo R & Miller R. Pregnancy complicated by severe preeclampsia and thrombocytopenia in a patient with scleroderma. Anesthesia and Analgesia 1997; 85: 839–41.CrossRef,PubMed,CAS,Web of Science® Times Cited: 2.
9. Zoey Sarah Dempsey, Simone Rowell, Rose McRobert, The role of regional and neuroaxialanesthesiain patients with systemic sclerosis. Local and Regional Anesthesia 2011:4 47–56.
10. Black CM. Scleroderma — systemic sclerosis. In: Cameron S, Davison AM, Grünfeld JP, Kerr D, Ritz E, eds. Oxford Textbook of Clinical Nephrology. Oxford: Oxford University Press, 1992: 667–77.
11. Redman CWG. Hypertension. In: de Swiet M, ed. Medical Disorders in Obstetric Practice. Oxford: Blackwell Science, 1995: 182–225.
12. Kanter G, Barash PG. Undiagnosed scleroderma in a patient with adifficult airway. Yale J Biol Med. 1998;71(1):31–33.
13. Smith GB, Shribman AJ. Anesthesia and severe skin disease.Anaesthesia.1984;39(5):443–455.
14. Roberts JG, Sabar R, Gianoli JA, Kaye AD. Progressive systemicsclerosis: clinical manifestations and anesthetic considerations. J ClinAnesth. 2002;14(6):474–477.
15. Thompson J, Conklin K. Anesthetic management of a pregnant patientwith scleroderma. Anesthesiology. 1983;59(1):69–71.
16. Sweeney B. Anaesthesia and scleroderma. Anaesthesia. 1984;39(11):1145.
17. Edmunds MR, Kyprianou I, Amissah-Arthur KN, Smith G. Elevatedintra-ocular pressure after sub-Tenon’s anaesthesia in systemic sclerosis.Anaesthesia. 2010;65(3):313–314.
18. Erk G, Taspinar V, Donmez F, Ornek D. Neuroaxialanesthesia in apatient with progressive systemic sclerosis; a case presentation andreview of the literature on systemic sclerosis. BMC Anesthesiol.2006;6:11.
19. Garcia-Sanchez MJ, Galdo-Abadin JR, Palacio-Rodriguez MA, et al.Anaesthetic management of a pregnant patient with CREST syndrome.Int J ObstetAnesth. 1999;8(2):146–147.
| How to Cite this Article: Shalu P S. A rare case of systemic sclerosis and its anaesthetic implications. Journal of Anaesthesia and Critical Care Case Reports July – Sep 2015; 1(1):12-15. |

{kind=link}
(Abstract) (Full Text HTML) (Download PDF)