Vol 9 | Issue 3 | September-December 2023 | Page: 21-22 | Cherian Roy, Rohit Kumar Patnaik, Samir Samal, Shakti Bedanta Mishra, Nupur Karan
DOI: https://doi.org/10.13107/jaccr.2023.v09.i03.227
Submitted: 04/03/2023; Accepted: 25/05/2023; Published: 10/09/2023
Author: Cherian Roy [1], Rohit Kumar Patnaik [1], Samir Samal [1], Shakti Bedanta Mishra [1], Nupur Karan [2]
[1] Department of Critical Care Medicine, Institute of Medical Sciences and SUM Hospital, Bhubaneswar, Odisha, India
[2] Department of Anaesthesia, Kalinga Institute of Medical Sciences, Bhubaneswar, Odisha, India
Address of Correspondence
Dr. Nupur Karan,
Department of Anaesthesia, Kalinga Institute of Medical Sciences, Bhubaneswar, Odisha, India
E-mail: nupurkaran2989@yahoo.com
Short Communication
Introduction
Long Covid has been recognized as a distinct entity with thrombotic sequelae [1]. Persistent systemic vascular inflammation caused by thrombosis drives the complications associated with long COVID. The risks of arterial and venous thrombosis after COVID-19 extend well beyond the hospitalization period. Early prophylactic anticoagulation has been shown to reduce the incidence of post-covid thrombotic sequelae [2]. Some evidence suggests the use of a higher than prophylactic dose for primary venous thromboembolism prophylaxis, especially in patients with a history of venous thromboembolism (VTE) [1]. We present a case of long Covid who developed recurrent thrombosis despite being on a therapeutic dose of anticoagulation.
Case Presentation
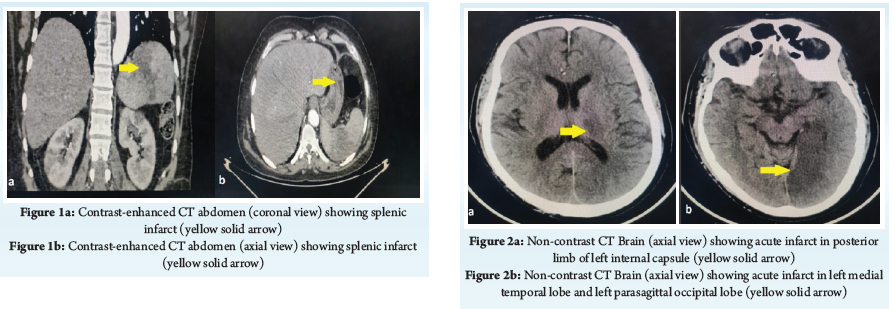
A 55-year-old male was brought to our Emergency Department with complaints of diffuse abdominal pain and black-coloured stools for three days. Contrast-enhanced CT abdomen (CECT) showed distal superior mesenteric artery (SMA) thrombosis and splenic infarct (Figure 1). He was treated for mild Covid-19 infection three months back. History also revealed he was hospitalized two months ago with a diagnosis of non-ST segment elevated myocardial infarction (NSTEMI) and acute ischemic stroke (Figure 2), which was managed with antiplatelets, statins and anticoagulants. He was discharged on oral anticoagulants (Tab Rivaroxaban 15 mg twice daily) for three months and was on regular follow-up. There was no history of smoking or hypertension. Protein C, Protien S, homocysteine levels were normal. After the diagnosis of SMA thrombosis, his anti-coagulation was increased to Tab Rivaroxaban 20 mg twice daily. No further thrombotic episodes have been noted as of date.
Discussion
This case suggests that unexplained repeat thrombotic events at multiple sites may have been a consequence of Covid-19 infection. Covid-19 patients experience both arterial and venous thromboembolism [3]. Most commonly, the former presents as myocardial infarction and ischemic stroke, whereas the latter as deep venous thrombosis and pulmonary embolism. Mechanisms include changes in lung structure secondary to chronic hypoxia, persistent immune dysfunction, and endothelial damage [1]. Risks of thrombotic events after mild Covid-19 are less clear, with the need and intensity of prophylactic anti-coagulation in this subset of patients being a matter of future research [4]. Shabaka et al. have shown that patients with a history of Covid-19 infection and previous thromboembolic events were at higher risk of developing a repeat thrombotic event [5]. Physicians need to be vigilant about the thrombotic events in patients with long Covid, even in patients receiving therapeutic anti-coagulation. Such patients require more frequent monitoring for signs of thrombotic events, risk factor management, and adherence to preventive therapies [3].
References
1. Wang C, Yu C, Jing H, Wu X, Novakovic VA, Xie R, et al. Long COVID: The Nature of Thrombotic Sequelae Determines the Necessity of Early Anticoagulation. Front Cell Infect Microbiol. 2022 Apr 5;12:861703.
2. Li P, Zhao W, Kaatz S, Latack K, Schultz L, Poisson L. Factors Associated With Risk of Postdischarge Thrombosis in Patients With COVID-19. JAMA Netw Open. 2021 Nov 22;4(11):e2135397.
3. Knight R, Walker V, Ip S, Cooper JA, Bolton T, Keene S, et al. Association of COVID-19 With Major Arterial and Venous Thrombotic Diseases: A Population-Wide Cohort Study of 48 Million Adults in England and Wales. Circulation. 2022 Sep 20;146(12):892–906.
4. Houchen-Wolloff L, Poinasamy K, Holmes K, Tarpey M, Hastie C, Raihani K, et al. Joint patient and clinician priority setting to identify 10 key research questions regarding the long-term sequelae of COVID-19. Thorax. 2022 Jul;77(7):717–20.
5. Shabaka A, Gruss E, Landaluce‐Triska E, Gallego‐Valcarce E, Cases‐Corona C, Ocaña J, et al. Late thrombotic complications after SARS‐COV ‐2 infection in hemodialysis patients. Hemodialysis International. 2021 Oct;25(4):507–14.
| How to Cite this Article: Roy C, Patnaik RK, Samal S, Mishra SB, Karan N. Post-COVID thrombotic sequelae: Once bitten, twice shy! Journal of Anaesthesia and Critical Care Case Reports. September-December 2023; 9(3): 21-22. https://doi.org/10.13107/jaccr.2023.v09.i03.227 |
(Full Text HTML) (Download PDF)