Vol 2| Issue 1 | Jan – Apr 2016 | page:2-3 | Aparna Sinha [1].
Author: Dr. Aparna Sinha [1].
[1] Institute of Minimal Access, Metabolic and Bariatric Surgery Max Healthcare, Saket, New Delhi.
Address of Correspondence
Dr Aparna Sinha
Associate Director and Senior Bariatric Anesthesiologist.
Institute of Minimal Access, Metabolic and Bariatric Surgery Max Healthcare, Saket,
New Delhi.
Email: apsin@hotmail.com
Obstructive Sleep Apnea: the growing Menace!!
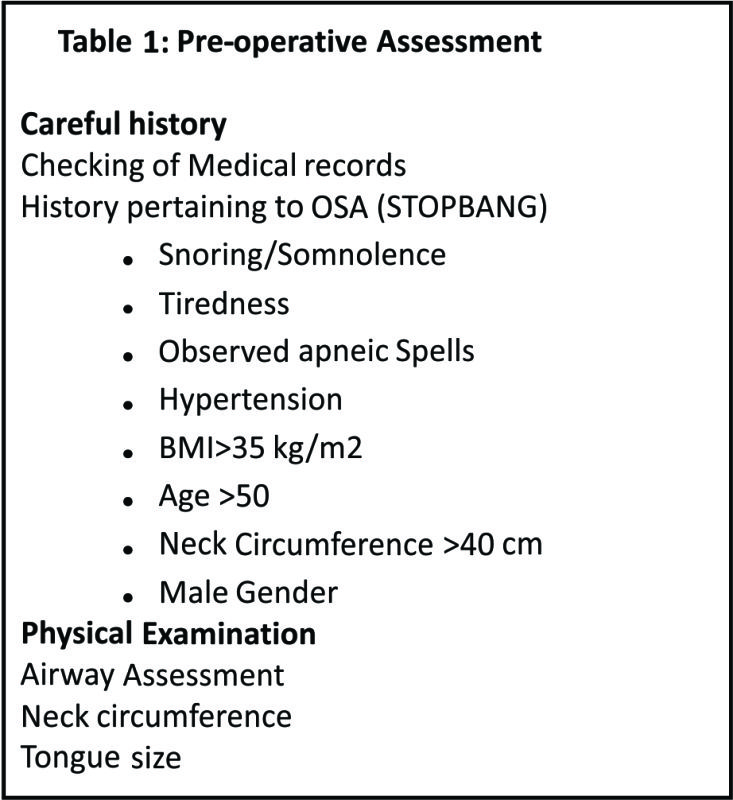
The medical and societal implications of the demographic transition which is leading to an alarming rise in obesity are significant and distressing. The rising prevelance of obstructive sleep apnea (OSA) can be considered to be a part and parcel of the obesity epidemic, and it is estimated that almost 90% sleep apneics are obese. In the last decade, sleep related disorders have attracted considerable attention of anesthesiologists from perioperative outcome perspective. Though, the impact of obesity is multi-dimensional; its impact on airway architecture and upper airway function is of prime importance to the anesthesiologist and has been widely substantiated in the existing literature. Obesity has emerged as the most significant risk factor in development of obstructive sleep apnea (OSA) and the exponential trends in obesity parallel the increasing prevelance of OSA. What is of equal concern is the strong link between OSA and cardiometabolic disorders. It is vital for the anesthesiologist and perioperative caregiver to be mindful of these facts, as they have direct influence on patient outcome and the utilization of healthcare resources. Moreover, another major fact that needs to be highlighted is that the rising trends in obesity are greater in the higher BMI segments, implying greater increase in patients who are super obese and super-super obese. By definition, OSA is a disorder which is characterised by an increase in oropharyngeal soft tissue that periodically blocks the airway during sleep, it can be expected that obesity and OSA, owing to increase in soft tissue mass, have been closely linked. It is estimated that upto 20% of middle-aged adults are suffering from OSA, however, it is feared that about 80% of female population and up to 93% of male populations remain undiagnosed. OSA has been implicated in the pathophysiology of several disease processes ranging from hypertension, congestive heart failure, arrhythmias, metabolic disorders and even pulmonary hypertension. Moreover, OSA might be associated with multiple comorbidities such as myocardial ischemia, heart failure, arrhythmias, cerebrovascular disease, metabolic syndrome, insulin resistance, gastroesophageal reflux, and obesity. The importance of diagnosing OSA in the preoperative period is due to the fact that the sleep apneic obese are at an increased risk for perioperative adverse events. These range from failure to extubate to hypoxemic events requiring reintubation, unplanned ICU admission, bleeding, atelectasis, hypotension, venous thromboembolism and aspiration with chest infection, to name a few. These events are higher in patients with greater periods of nocturnal hypoxemia. Overall, in these patients there is an increased risk for hypoxemic events in the perioperative period. These events are higher in patients who exhibit with greater periods of nocturnal hypoxemia. The postoperative pathophysiological changes and persistent drug effects after general anesthesia have a negative effect on the symptoms of sleep apnea. Given the vast majority of undiagnosed OSA, it is imperative that anesthesia providers familiarise themselves with its clinical presentation and methods to diagnose OSA. The perioperative events are mostly related to compromised oxygen reserves, difficult airway management, opioid related misadventures and airway obstruction. The other events can be experienced in the form of biventricular failure, systemic and pulmonary hypertension. Conventionally, overnight polysomnography (PSG) is the gold standard for diagnosing OSA. This relies on estimation of Apnea Hypopnea Index (AHI) per hour of sleep to determine the presence and severity of OSA, where apnea refers to cessation of airflow for 10 seconds, and hypopnea is reduced airflow with greater than 4% fall in oxygen saturations. As per American Academy of Sleep Medicine (AASM), diagnosis of OSA requires either an AHI ≥15, or AHI ≥5 with symptoms, such as daytime sleepiness, loud snoring, or observed obstruction during sleep. OSA is considered mild if AHI 5 to 15, moderate if AHI 15 – 30, and severe for AHI >30. It is estimated that 82% of men and 92% of women with moderate-to-severe sleep apnoea have not been diagnosed. A very high index of suspicion needs to be maintained to allow timely detection and optimisation. It may not be practical to subject every patient to PSG. However, owing to wide prevalence of OSA the use of preoperative screening tools should help to identify the patients with sub-clinical and undiagnosed OSA. Chung et al designed a preoperative screening tool called as the STOP Bang questionnaire, which has been further validated and is suggested as a part of routine preoperative assessment. In this model, there are eight questions, a YES to each question is scored as 1 and the maximum score is eight (8). It has high sensitivity at a score of ≥3, and the questionnaire is considered helpful to identify patients having moderate and severe OSA (Table 1). The same has been validated in several trials. Higher BMI segment patients have more serious consequences on their respiratory systems. The most dreaded of these remains the development of obesity hypoventilation syndrome (OHS), which is marked by daytime sleepiness, associated with alveolar hypoventilation (pCO2>45 mmHg). Prevalence of daytime hypercapnia (OHS) proportionately increases with increasing BMI (from 20 to 50 % in superobese patients). Anesthesiologists need to be mindful of the growing prevalence of Obesity hypoventilation, which is a serious condition that can lead to significant adverse outcomes in the perioperative period, including mortality. Anesthesiologist plays a very important role in timely detection and management of sleep disorders. In OHS, in addition to chest wall restriction, the compensatory mechanism that should maintain ventilation is impaired. The most immediate method to manage and revere the respiratory failure associated with such disorders is positive airway pressure (PAP) therapy.
Conclusion
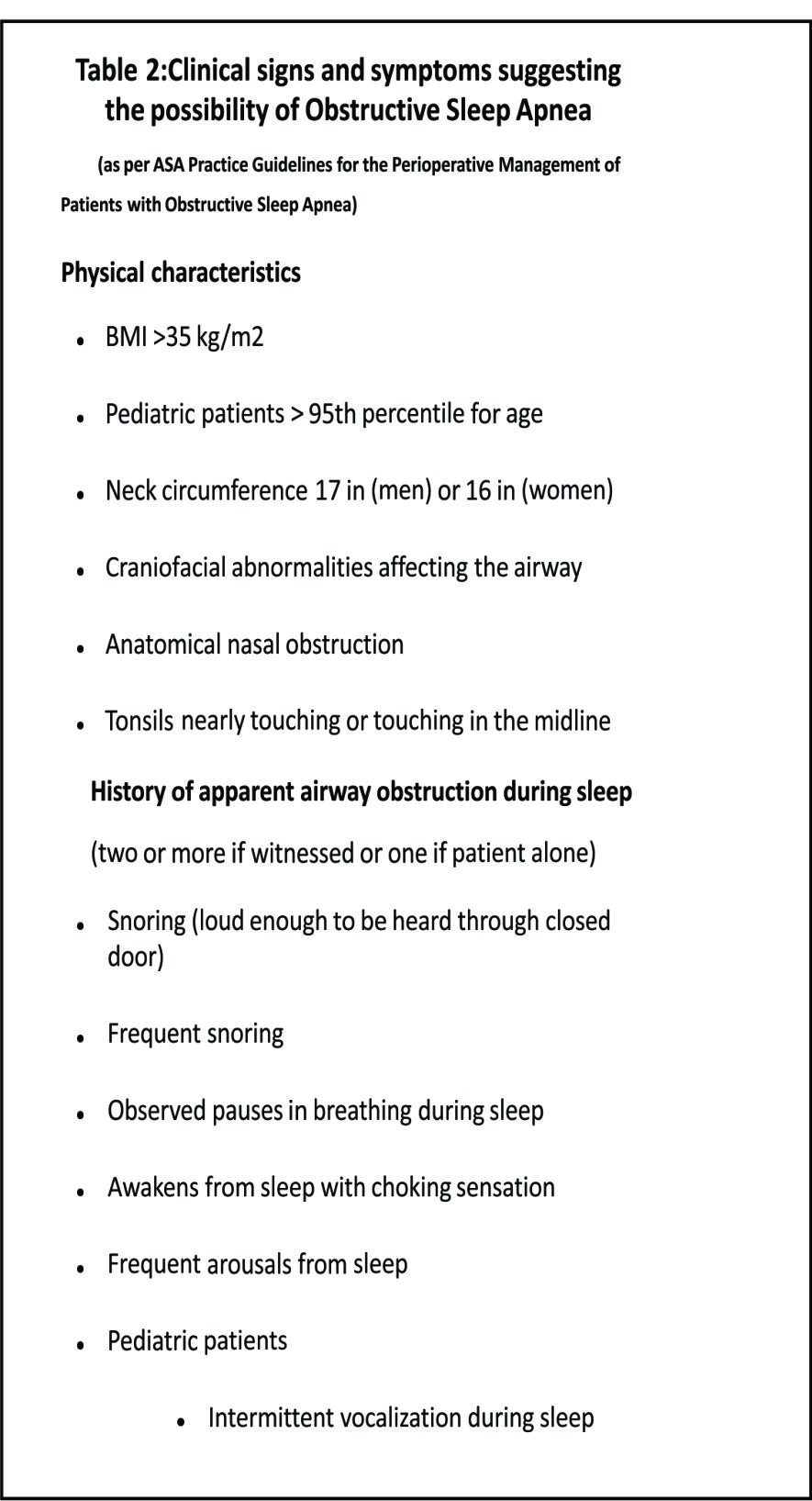
We, as perioperative physicians, are involved in perioperative care not just for surgical patients but also for procedural sedation, anesthesia at remote location, patients in triage, being transported to the hospital and postoperative care that continues even after discharge. Caution needs to be exercised particularly in day care settings, keeping a very high index of suspicion. It’s extremely crucial to familiarize ourselves with the screening tools and the practice guidelines issued by ASA (Table 2).
The ever-increasing prevalence of obstructive sleep apnea demands simplistic method to detect, diagnose and manage in the ambulatory settings. Anesthesiologists have the most vital role in detecting OSA in surgical population, optimising them in preoperative period and preventing any perioperative catastrophe.
Aparna Sinha
References
1. Sturm R. Increases in morbid obesity in the USA: 2000-2005. Public Health2007; 121:492e6.
2. Shamsuzzaman AS, Gersh BJ, Somers VK. Obstructive sleep apnea: implicationsfor cardiac and vascular disease. JAMA 2003; 290:1906e14.
3. Andreyeva T, Sturm R, Ringel JS. Moderate and severe obesity have largedifferences in health care costs. Obesity 2004; 12:1936e43.
4. Berg G, Delaive K, Manfreda J, Walld R, Kryger MH. The use of health-careresources in obesity-hypoventilation syndrome. Chest 2001; 120:377e83.
5. Young T, Peppard PE, Gottlieb DJ (2002). Epidemiology of obstructive sleep apnea: a population health perspective. Am J Respir Crit Care Med 165: 1217-1239.
6. Shepard JW Jr (1992) Hypertension, cardiac arrhythmias, myocardial infarction, and stroke in relation to obstructive sleep apnea. Clin Chest Med 13: 437-458.
7. Hwang D, Shakir N, Limann B, Sison C, Kalra S, et al. (2008) Association of sleep-disordered breathing with postoperative complications. Chest 133: 1128-1134.
8. Kaw R, Chung F, Pasupuleti V, Mehta J, Gay PC, et al. (2012) Meta analysis of the association between obstructive sleep apnoea and postoperative outcome. Br J Anaesth 109: 897-906.
9. Chung F, Yegneswaran B, Liao P, et al. STOP questionnaire: a tool to screen patients for obstructive sleep apnea. Anesthesiology 2008; 108: 812–21.
10. Chung F, Yegneswaran B, Liao P, et al. Validation of the Berlin questionnaire and American Society of Anesthesiologists checklist as screening tools for obstructive sleep apnea in surgical patients. Anesthesiology 2008; 108: 822–30.
11. Finkel KJ, Searleman AC, Tymkew H, et al. Prevalence of undiagnosed obstructive sleep apnea among adult surgical patients in an academic medical center. Sleep Med 2009; 10: 753–8.
| How to Cite this Article: Sinha A. Obstructive Sleep Apnea: the growing Menace!!. Journal of Anaesthesia and Critical Care Case Reports Jan-Apr 2016; 2(1):2-3. |