Vol 2 | Issue 2 | May-Aug 2016 | page: 13-15 | Mamta Jain, Suchita Lahiri, Arun Puri, Anish Singh.
Authers: Mamta Jain[1], Suchita Lahiri[1], Arun puri[1], Anish Singh[1].
[1] Department of Anaesthesiology, Max Superspecialty Hospital, Patparganj New Delhi, India.
Address of Correspondence
Dr. Mamta Jain
Department of Anaesthesiology, Max Superspecialty Hospital, I.P Extension
Patparganj New Delhi,
India – 110092.
Email: mamtajainsingh@gmail.com
Abstract
Introduction: The increasing prevalence of the use of enteral feeding tubes in postoperative patients and in critical care settings pose a potential for malposition of the tube which may result in several complications.
Case Report: The chances of malposition are increased in cases where glottic reflexes are blunted. These malpositioned nasogastric feeding tubes are not included in risk management databases, therefore they may be underreported. Recent data suggest that malpositioned blindly, inserted feeding tubes may cause serious thoracic complications in mechanically ventilated patients.
Conclusion: We report a case in which a misplaced nasogastric tube was found to be the cause of an unusual ventilator leak.
Key Words: Nasogastric tube; malposition; ventilator leak; thoracic complications.
Introduction
Nasogastric tube (NGT) may be used for stomach lavage, and enteral nutrition in critically ill patients. The insertion of NGT is usually easy and requires little training. However, NGT placement may cause severe respiratory complications, esophageal perforation and tracheal injury. Placement of NGT is confirmed by several methods like auscultation, aspiration of gastric content, measuring pH of gastric content, capnography and chest X-ray.
Case report
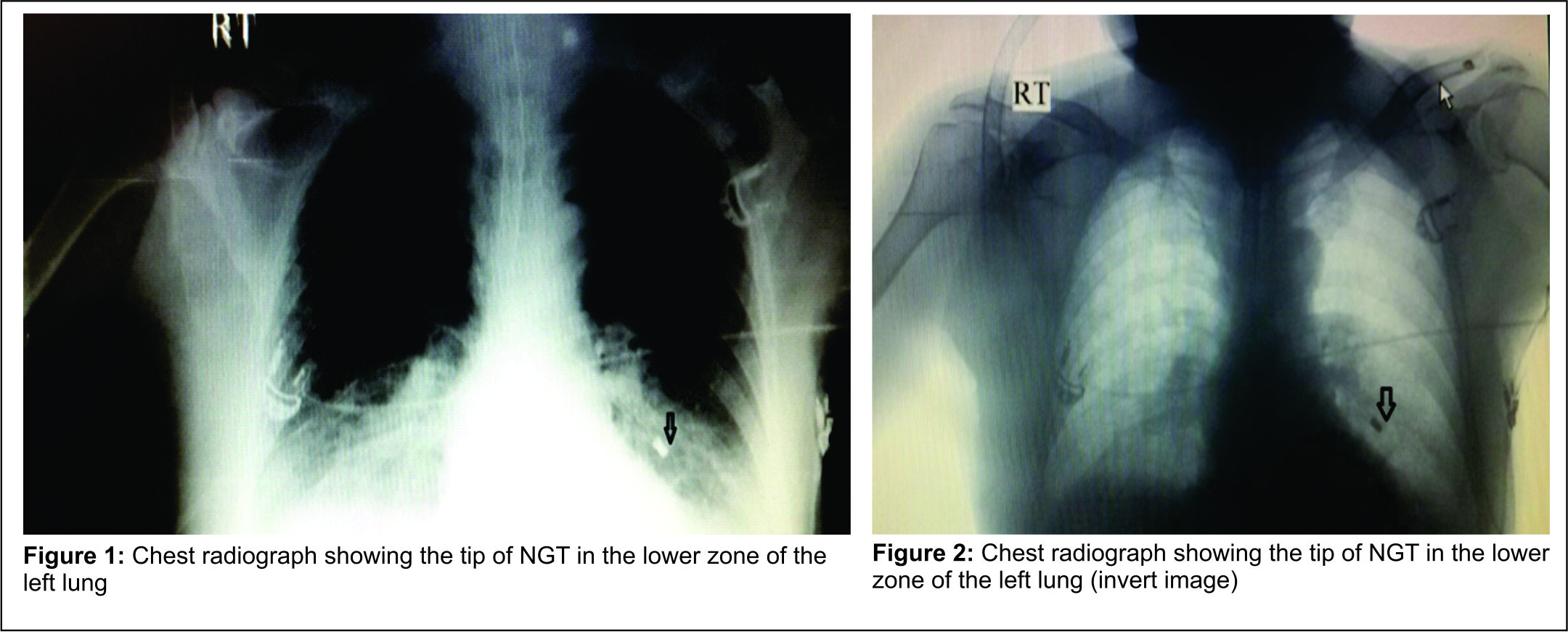
A 65-year-old male patient, who was a known case of maxillary carcinoma with complaints of recurrence of growth, was planned for total maxillectomy. He had previously undergone maxillectomy six months back and had undergone radiotherapy and chemotherapy about a year back. His malampatti grade was Grade IV and mouth opening was less than two fingers. Awakefibre-optic nasal intubation was conducted in this patient. A nasal flexometallic endotracheal tube of 7.0 mm internal diameter was inserted and secured with tapes. Anesthesia was maintained with 0.6% isoflurane in a 40% oxygen and 60% nitrous oxide mixture and inj. Vecuronium. NGT was inserted after induction but was found to be in the oral cavity. After surgery, NGT insertion was reattempted. On auscultation at the epigastric area, a faint gurgling sound was heard and the patient was shifted to ICU being hand ventilated with a Bain’s circuit. In the ICU, the patient was kept on ventilatory support (volume control mode). Parameters set were Vt 500, frequency 12 breaths/min, PEEP 5, FiO2 0.4. It was noted that adequate tidal volume was not being delivered to the patient. The expired tidal volume was noted to be approximately 250 ml lower than the preset tidal volume. It was a significant leak which was immediately assessed. All circuit connections were checked and were found to be secure. An occasional leak was audible at the mouth and 2-3 ml of additional air was added to the cuff of the tracheal tube. Cuff pressure was 25mm Hg. But the problem persisted. After ruling out all obvious causes, it became apparent that the source of the leak was the NGT, through which the air was coming out. An urgent chest radiograph was performed and the NGT was found to be in the lung (figure 1& figure 2 : Chest radiograph showing the nasogastric tube in left lower lung). Repositioning of the NGT resolved the situation. The ventilator leak was minimal and the patient was adequately ventilated.
In this case, it was mistakenly assumed that the NGT was in the stomach because it had advanced without resistance. There was no instance of kinking or coiling of the tube in the oropharynx and auscultation test was positive though faint. The patient was followed up and discharged after a week. He didn’t suffer from any respiratory complications.
Discussion
Nasogastric tube feeding is a common practice in many clinical conditions. Many patients in whom these tubes are required are seriously ill, and have impaired cough and gag reflexes [1]. These patients are at an increased risk of misplacement of nasogastric tubes. The incidence of a misplaced nasogastric tube in the airway ranges from 0.3% to 15% and is more common after chest trauma or in patients who are mechanically ventilated [2]. Large volume low pressure cuffs used in the intensive care settings cause less mucosal compression and necrosis and reduce some of the complications associated with long term intubation [2]. However, because these cuffs are softer than the low volume high pressure cuffs and remain wrinkled even when inflated, NGT may in rare cases be introduced into the trachea (especially rigid wire-guided or narrow bore tubes) [2,3]. Moreover, endotracheal misplacement of a narrow-bore nasogastric feeding tube can be facilitated by endotracheal tubes that are large as compared to the tracheal lumen or have a small cuff diameter to tracheal diameter ratio [4]. When the NGT is placed and an aspirate with a pH <5 is not obtained, then a chest radiograph is regarded as the gold standard to verify correct tube placement. However, interpreting supine chest radiographs in critically-ill patients may be difficult [5]. When in doubt, the best practice is to use a radiograph to check the tube’s location [6]. A chest radiograph including the upper half of the abdomen should be done in all patients who have swallowing problems, confused patients and those in ICU to verify the tube’s intra-gastric position. The tip of the tube can be seen as a white radio-opaque line and should be below the diaphragm on the left side. A two-step insertion of a nasogastric feeding tube has been tested by Mardestein et al. [7]. These authors applied a protocol which required a pause when the NGT has reached 35cm, so that a radiograph could confirm that the tube had not been placed in a bronchus. If the tube was determined to be in the esophagus, it could safely be advanced. A second chest radiograph was performed when the NGT was inserted unto the desired length to verify its position in the stomach.
Although, this approach had been initially proposed by Roubenoff et al., it had not been tested until Mardestein et al. They reported that with the two step approach system, no tube placed in the esophagus had caused pulmonary damage [7,8]. The post-intervention incidence of pneumothorax among patients having an intrabronchial feeding tube has been reduced to 3.3% from the pre-intervention rate of 26.9%. Sorokin et al. applied a policy to reduce incidences of pneumothorax caused by NGT that are inserted in intubated or sedated patients [9]. They incorporated three changes: 1) Only experienced doctors were allowed to insert NGT in intubated or sedated patients, a safer tube was used and a two-step method of insertion was evaluated for its efficacy in difficult cases. The tubes were either not advanced beyond 35 cm or until a radiograph was obtained or were advanced under direct laryngoscopic, fluoroscopic or capnometric guidance. 2). The feeding tubes malpositions and related complications [10] were monitored and reported regularly to the clinical staff and 3) Resident education program on feeding tube insertion was started [7].
Conclusion
The take home message in this case clearly illustrates how a misplaced NGT may interfere with ventilation [11]. It is especially useful to remember this complication when a NGT cannot be placed under direct vision. A fibreoptic confirmation of the NGT intra-operatively can be very useful especially where intra oral surgery is performed and anatomy is likely to be distorted post operatively. In addition, leaks between the breathing system and the patient are much more reliably detected by expired volume monitoring than by a ventilator alarm [12]. This case also illustrates that if the leak hadn’t been detected it could have led to the dreaded complication of aspiration pneumonitis if feeding was commenced [13]. A chest radiograph still remains the Gold Standard for detection of misplaced NGT till future studies evaluate other cheaper and non-invasive modalities for the same.
References
. Raff MH, Cho S, Dale R. A technique for positioning nasoenteral feeding tubes. J parenter and Enteral Nutr 1987;11:210-213.
2. Elpis G, Kevin J. Blindly inserted nasogastric feeding tubes and thoracic complications in intensive care. Health 2010;2(10):1135-41.
3. Dorsch JA, Dorsch SE. Understanding anaesthesia equipment. 5th ed. Chapter 19 Tracheal tubes and associated equipment, 577.
4. Wang PC, Tseng GY, Yang HB, Chou KC, et al. Inadvertent tracheobronchial placement of feeding tube in a mechanically ventilated patient. Journal of the Chinese Medical Association 2008;71(7):365-367.
5. Thomas B, Cummin D, Falcone RE. Accidental pneumothorax from a nasogastric tube. N Engl J Med 1996;335:1325–6.
6. Stock A, Gilbertson H, Babl FE. Confirming nasogastric tube position in the emergency department: pH testing is reliable. Pediatr Emerg Care 2008;24(12):805-9.
7. Mardestein, E.I., Simmons, R.L. and Ochoa, J.B. Patient safety: Effect of institutional protocols on adverse events related to feeding tube placement in the critically ill. Journal of the American College of Surgeons 2004;199(1):41-47.
8. Roubenoff, R. and Ravich, W. Pneumothorax due to nasogastric feeding tubes. Archives of Internal Medicine 1989;149(2):184-186.
9. Sorokin, R. and Gottlieb, J. Enhancing patient safety during feeding tube insertion: A review of more than 2000 insertions. Journal of Parenteral and Enteral Nutrition 2006;30(5):440-445.
10. Jens S, Thomas H, Sebastian F and Sandra Riede. Bronchopulmonary Complications of Nasogastric tube Placement. Global Journal of Respiratory Care 2014;1:13-16.
11. Tenholder M, Erwin W and Nelson H. Lost tidal volume in a 71-year old ventilated patient. Chest 1994;106(6):1869-1871.
12. Sykesm K. Essential monitoring. British Journal of Anaesthesia 1987;59:901-12.
13. Monish S, Sandeep J, Arun M. Malposition of a nasogastric tube. Annals of Cardiac Anaesthesia 2015;18(2):272-273.
| How to Cite this Article: ain M, Lahiri S, Puri A, Singh A. Nasogastric tube malposition leading to a ventilator leak: a case report. Journal of Anaesthesia and Critical Care Case Reports May-Aug 2016; 2(2): 13-15. |
