Vol 4 | Issue 3 | Sep-Dec 2018 | page: 7-8 | Muralidhar Thondebhavi
Authors: Muralidhar Thondebhavi [1].
[1] Department of Anaesthesiology and Pain Management Apollo Speciality Hospital, Bangalore.
Address of Correspondence
Dr. Muralidhar Thondebavi,
Consultant, Anaesthesiology and Pain Management Apollo Specialty Hospital, Bangalore
E-mail: muralidharts@googlemail.com
Mental models, to put in simple words, are the representation of how anything works (from Smartphone to complex financial systems). We cannot carry the complexity of the world we inhabit, and hence simplify it through mental models into easily understandable concepts. This helps us reason, judge and take better decisions. Each field of study has a set of most important principles on which the foundations of that discipline are built on. They form the key mental models which should be incorporated for better decision making. The quality of thinking and decision making is proportional to the number of good quality mental models we carry in our head. This equates to more tools in our mental toolbox and hence more options to deal with a certain problem. Many of us consider ourselves specialists. Instead of a collection of mental models, we have a few from our field. A psychologist thinks in incentives, an engineer in systems and a mathematician in algorithms. They, as specialists are limited to thinking in one way to solve a problem. By incorporating these three disciplines in our head, we can tackle a problem in a multidimensional way. This decreases the blind spots and improves decision quality. Just carrying few models in our head will not make a difference. Arranging them in a nice latticework is paramount. Learning should take place with this framework in the head and we should make it a lifelong project to acquire more models as we go along. As doctors, in general, we are limited to our field and resist learning mental models from other unrelated fields. However, there are
some general mental models which can be learnt easily such as ‘circle of competence’, ‘map is not the territory’, ‘first principles thinking’, ‘thought experiment’, ‘second order thinking’ and ‘inversion’. I would like to highlight a few models with examples: – Model of ‘Circle of Competence’ teaches us to know the perimeter of things that we know how to perform with high confidence (Eg: Intubation in a patient with easy airway for consultant anaesthesiologist). We have to stay within this circle and try to expand it by training. Outside this inner circle lies a dangerous zone wherein “we think we know” and trying to do things here leads to disaster (Eg: Trying to use a new airway tool in a difficult airway situation without appropriate training). – Model of ‘First Principles Thinking’. Unless we understand the basic concepts of ‘why’ we do certain things we cannot execute high quality care for our patients. An example is not understanding the physiological basis of preoxygenation and just concentrating on the time prescribed in the text books for the same. This might lead to inadequate preoxygenation in certain group of patients. This model also highlights the need to impart first principles concepts during the training period with emphasis on understanding ‘why’ we do rather than ‘what and how’ we do. – Model of ‘Compounding’. This is an important model of the finance world and describes a process by which interest added to fixed sum earns interest and the newly added interest earns more interest and this continues ad infinitum. This is an exponential process and can be applied to
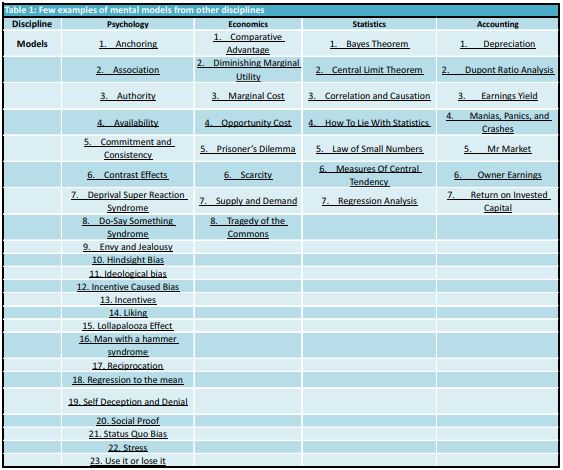
non-financial aspects. An example is health of an individual. A regular exercise program and good diet regimen practised on a daily basis leads to better health as the years progress. Another example is learning. Reading 10-20 pages a day has a compounding effect on learning. – Model of ‘Map is not the territory’. A map is an imperfect representation of reality. They are reductions of what they represent. They also represent a snapshot of a point of time and hence may depict something that no longer exists. A difficult airway algorithm is a map. However, every scenario of difficult airway rarely behaves as the algorithm suggests (not mentioning the emotions and mental trauma omitted in the guideline). A simulation training program probably narrows this gap by bringing reality closer to a learning mind and in turn circumventing the limitations of just a ‘map’ . Having explored a few models in brief, it is important to embark on a journey to learn and internalise more models (Table 1). ‘The more the merrier’ aphorism will not be wrong if we build a strong latticework of models to understand the world around us and in turn improve the decision making skills. This will make us better clinicians, better human beings and definitely improve patient care.
References
- 1. Poor Charlie’s Almanack: The Wit and Wisdom of Charles T. Munger: Charles T. Munger, Peter D. Kaufman, Warren E. Buffett 2. Seeking Wisdom: From Darwin to Munger, 3rd Edition: Peter Bevelin 3. A Lesson on Elementary, Worldly Wisdom As It Relates To Investment
Management & Business (https://old.ycombinator.com/munger.html) 4. https://fs.blog/mental-models/ 5. https://jamesclear.com/mental-models 6. https://www.safalniveshak.com/mental-models/
| How to Cite this Article: Thondebavi M. Mental Models and the Anaesthetist. Journal of Anaesthesia and Critical Care Case Reports Sep-Dec 2018; 4(3):7-8. |
