Vol 9 | Issue 3 | September-December 2023 | Page: 02-05 | Vivek Sharma, Hiteshi Aggarwal, Vivek Prakash, Pallavi Ahluwalia
DOI: https://doi.org/10.13107/jaccr.2023.v09.i03.221
Submitted: 10/03/2023; Accepted: 21/06/2023; Published: 10/09/2023
Author: Vivek Sharma [1], Hiteshi Aggarwal [1], Vivek Prakash [1], Pallavi Ahluwalia [1]
[1] Department of Anaesthesia, Teerthanker Mahavir Medical College and Research Centre, Delhi Road, NH 24, Bagadpur, Moradabad, Uttar Pradesh, India.
Address of Correspondence
Dr. Hiteshi Aggarwal,
Department of Anaesthesia, Teerthanker Mahavir Medical College and Research Centre, Delhi Road, NH 24, Bagadpur, Moradabad, Uttar Pradesh, India.
E-mail: Hiteshiaggarwal29@gmail.com
Abstract
Introduction: Transurethral resection of bladder tumors (TURBT) is the first-line method and mainstay for endoscopic diagnosis, staging, and treatment of urinary bladder tumours. Hypotonic fluid absorption, electrolyte imbalance from irrigation, haemorrhage, and obturator jerk episodes are just a few of the procedure’s intrinsic risks. Cardiovascular issues were more likely to arise in elderly patients undergoing this surgery. A high risk of pulmonary oedema, arrhythmia, and bleeding problems exists in individuals with coronary artery disease (CAD), dilated cardiomyopathy (DCMP), multiple comorbidities, and anticoagulant medication.
Case Presentation: Here, we provide a challenging situation of A 74-year-old man was scheduled to have TURBT (Transurethral Resection of Bladder Tissue) for a bladder mass with hematuria and many comorbidities, including Hypertension (HTN), Chronic obstructive pulmonary disease (COPD), coronary artery disease (CAD), post percutaneous transluminal coronary angioplasty (PTCA), cerebrovascular accident (CVA), dilated cardiomyopathy (DCMP), ejection fraction (EF) 25%, and Severe MR necessitating obturator nerve block (ONB), spinal anaesthesia (SA), and epidural anaesthesia (EA) for perioperative and postoperative anaesthetic as well as analgesia, which was effectively handled without any difficulties.
Conclusion: Elderly patient with ischemic cardiomyopathy are at higher risk of major cardiovascular events perioperatively. Low dose spinal anaesthesia combined with epidural anaesthesia provides better hemodynamic stability, prevents myocardial depression, provide perioperative analgesia and early ambulation.
Keywords: Obturator nerve block, Spinal anaesthesia, General anaesthesia practice, Transurethral Resection of Bladder Tissue (TURBT), Cerebrovascular accident (CVA), Chronic obstructive pulmonary disease (COPD)
Introduction:
Elderly patients often have cardiovascular and respiratory comorbidities with urological problems [1]. Ischemic heart disease is the leading cause of death in the world in patients undergoing major non-cardiac surgery. CAD is a primary risk factor for perioperative morbidity and mortality in patients with a fragile cardiovascular profile. Geriatric patients are at increased risk for perioperative major adverse cardiac events including arrhythmias, electrolyte imbalance, congestive heart failure, myocardial ischemia, and cardiac arrest [2]. The goal of anaesthesia management should focus on maintaining preload, reducing afterload, avoiding myocardial depressants, provide adequate analgesia, maintain hemodynamics stability and myocardial oxygen demand and supply [3]. Geriatric patients have age-related compromised organ reserve, chronic ailments and multiple comorbidities, results in postoperative complications [4].
Urosurgical procedures like transurethral resection of bladder tumor (TURBT), and transurethral resection of the prostate (TURP) require lithotomy position, which poses such patients further at risk of fluid overload and electrolyte imbalance such as hyponatremia and thus at increased risk of TURP syndrome. So, the choice of anaesthesia i.e., general anaesthesia, neuraxial and regional anaesthesia relies on preventing myocardial oxygen demand and supply mismatch [5, 6].
Here we report a successful anesthetic management of a geriatric patient with known dilated cardiomyopathy (DCMP), who underwent TURBT under combined low-dose spinal and epidural anaesthesia along with obturator nerve block.
Case Report
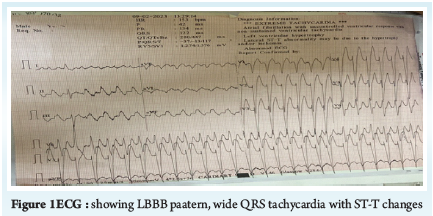
A 74-year-old patient, diagnosed case of bladder cancer, was planned for TURBT. The patient was a chronic smoker and was a known case of HTN, CAD, and DCMP with LBBB, who underwent percutaneous coroary intervention (PCI) 2 months back, not on regular medications. His METS score was less than 4 and breath holding time was < 15 seconds. Auscultation revealed occasional wheeze and fine basal crepitations bilaterally. Chest X-ray (Figure 2) findings suggested increased translucency of lung fields and prominent bronchovesicular marking in the lung fields. Transthoracic 2D Echo was suggestive of global hypokinesia, left ventricular ejection fraction of 20-25%, severe mitral regurgitation, moderate pulmonary hypertension, diastolic dysfunction grade II and a 12 lead ECG (Figure 1) was suggestive of left bundle branch block (LBBB) with significant ventricular ectopics. His chest CT reports suggested moderate to severe emphysematous changes with bronchial wall thickening with scattered areas of fibrosis and consolidation, suggestive of COPD changes. Preoperative hemoglobin was 9.5 g/dl. Preoperatively, the patient was on oral tablets like Doxyphylline, Amlodipine, Ivabradine, and Dytor.
The patient was classified as ASA grade IV and was planned for TUBT under combined low-dose spinal and epidural anaesthesia along with obturator nerve block. (Figure 2, 3)
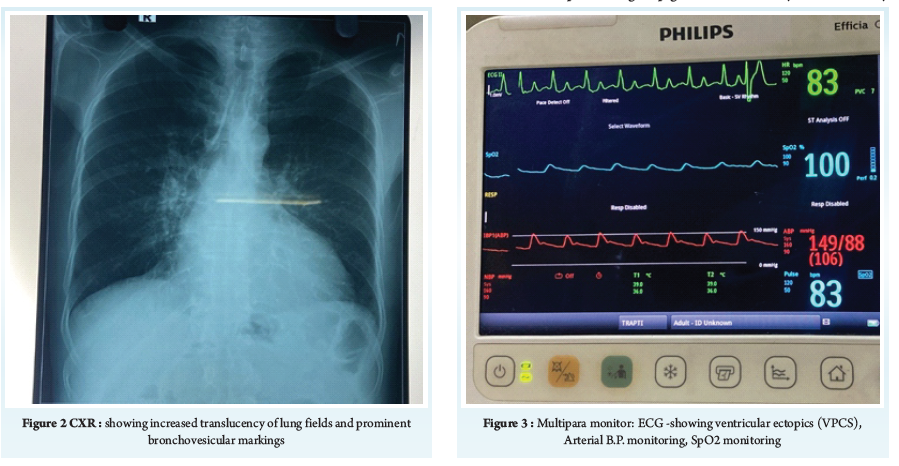
Intraoperatively, after establishing standard monitors (Figure 3) like electrocardiogram (ECG), non-invasive blood pressure (NIBP), SPO2 and securing a 16 G iv cannula, USG guided arterial line 20 G was secured in the left radial artery and invasive BP monitoring was established. Baseline vitals were IBP 120/76 mmHg, HR 84/min, SPO2 86%. Under asceptic precautions, an 18 G epidural catheter was inserted into the L3- L4 space, followed by spinal anaesthesia in the same space with the administration of 9 mg of injection levobupivacaine and 25 microgram fentanyl. USG guided bilateral obturator nerve block was performed using 10 mL of 0.5% bupivacaine (50 mg).
Block was achieved till T8 level and there was minimal decrease in BP from baseline with fall of less than 20% and HR was maintained at 80-90/min. A single episode of hypotension was recorded and was managed with inj. mephenteramine 1.5 mg i.v. bolus. We opted for a restricted fluid regime to avoid fluid overload and inj. Dytor 10 mg was administered at the end of the surgery. The patient was hemodynamically stable intraoperatively with no complaints of chest pain, sweating, or breathlessness. The surgery lasted for 90 minutes, and intraoperatively, MAP was maintained more than 65 mmHg and HR was maintained at 80-90/min and volume status was assessed using pulse pressure variation (PPV). Epidural loading of 0.125% 6 ml Bupivacaine was given at 90 minutes for post-operative analgesia. Recovery from spinal anaesthesia was assessed using modified Bromage scale and visual analog scores (VAS) were recorded. Postoperatively, injection paracetamol i.v SOS and epidural top-ups of 0.125% 6 ml bupivacaine was administered every 6 hours till 24 hours.
Discussion
Anaesthesia management of cardiac patients for non cardiac surgery solely relies on preventing myocardial oxygen demand and supply mismatch. Hemodynamic stability is important in geriatric patients with reduced cardiovascular reserve. Perioperative management of such patients requires preoperative evaluation, risk stratification, peri-operative monitoring, maintaining hemodynamic stability, and aims to provide adequate analgesia and early ambulation post-surgery [7].
Combined low-dose spinal anaesthesia plus epidural anaesthesia has better safety profile in patients with low cardiovascular reserve due to better hemodynamic stability. Compared to high dose spinal anaesthesia, low dose spinal anaesthesia leads to minimal decrease in systemic venous resistance (SVR), thus preventing hypotension and at the same time, decreasing afterload of left ventricle and thus, increasing cardiac output. Patients with ischemic heart disease and cardiomyopathy have increased sympathetic activity to maintain the cardiac output, and so are at increased risk of decrease in SVR with high dose spinal anaesthesia [8]. Cenkowski JM 2019 et al. showed that low-dose bupivicaine group gain faster recovery of the sensory and motor blockade, early discharge, and better patient satisfaction compared to high dose bupivacaine [9]. Alsaeid et al. also found that a small dose of heavy bupivacaine 0.5% (5 mg) provided better hemodynamic stability with minimal side effects in elderly patients [10]. Mehdi Sanatkar et al also showed hemodynamic stability and no ST-T changes with low dose of bupivacaine and sufentanil in patients with CAD [11]. Jain M et al reported use a low dose of a local anaesthetic and an opioid during a graded epidural anaesthesia in patients with IHD and low ejection fraction posted for nephrolithotomy and observed a stable hemodynamic profile with adequate postoperative analgesia [12].
Due to the large network of venous plexus in the prostate gland’s ability to absorb fluid, TURBT is often an hour-long treatment with an additional risk of fluid overload and TURP syndrome. As a result, TURP syndrome and congestive heart failure are more common in patients with cardiomyopathy. Patients undergoing TURBT has additional risk of bladder rupture due to stimulation of obturator nerve adjacent to lateral bladder wall by electrical current passing via rectoscope. USG guided obturator nerve block can prevent the obturator reflex and stimulation of adductor muscle [13]. Sharma D et al claim that using ONB and SA in TURBT is a very secure and reliable kind of anaesthesia to stop adductor contraction [14].
Local anesthetics have narrow margin of cardiovascular safety. Addition of adjuvants like opioids to low dose local anesthetics improves the safety margins in patients with poor cardiopulmonary reserve as, opioids have favorable cardiovascular profile in comparison to local anesthetics and thus preventing hypotension and myocardial depression [15].
Conclusion
Elderly patients with ischemic cardiomyopathy are at higher risk of major cardiovascular events perioperatively. Low dose spinal anaesthesia combined with epidural anaesthesia provides better hemodynamic stability, prevents myocardial depression, provide perioperative analgesia and early ambulation.
Clinical message
Multimodal triple approach using low-dose spinal anaesthesia with epidural anaesthesia and nerve blocks can help minimize major adverse cardiac events in geriatric patients with cardiac dysfunction.
References
1. Aceto P, Antonelli Incalzi R, Bettelli G, et al. Perioperative Management of Elderly patients (PriME): recommendations from an Italian intersociety consensus Aging Clin Exp Res. 2020;32(9):1647-1673.
2. Hedge J, Balajibabu PR, Sivaraman T. The patient with ischaemic heart disease undergoing non cardiac surgery. Indian J Anaesth 2017;61:705-11.
3. Regional Anaesthesia in the Patient Receiving Antithrombotic or Thrombolytic Therapy: American Society of Regional Anaesthesia and Pain Medicine Evidence-Based Guidelines (Fourth Edition) Regional Anaesthesia & Pain Medicine 2018;43:566.
4. Adigun TA and Sotunmbi PT. Combined Spinal Epidural Anaesthesia for TURP in a Nigerian Geriatric Patient with Low Ejection Fraction- Case Report. SM J Clin Med. 2017; 3(3): 1027.
5. Kabi A, Kumari R, Bone S. Transurethral resection of bladder tumor surgery conducted using Epidural anaesthesia and obturator nerve block in an elderly multimorbid male. J Clin Images Med Case Rep. 2021; 2(4): 1266.
6. Jain A, Jain K, Bhagat H, Mangal K, Batra Y. Anesthetic management of a patient with hypertrophic obstructive cardiomyopathy with dual-chamber pacemaker undergoing transurethral resection of the prostate. Ann Card Anaesth 2010;13:246-8
7. Tekgül ZT, Horsanali BÖ, Horsanali MO. Anaesthesia for Urological Surgery. Current Topics in Anesthesiology [Internet]. 2017 Feb 8
8. Kaul, Tej K.1; Tayal, Geeta2,. Anaesthetic Considerations in Cardiac Patients Undergoing Non Cardiac Surgery. Indian Journal of Anaesthesia 51(4):p 280-286, Jul–Aug 2007.
9. Cenkowski MJ, Maguire D, Kowalski S, Al Gurashi FA, Funk D. Hemodynamic effects of low-dose bupivacaine spinal anaesthesia for cesarean section: A randomized controlled trial. Saudi J Anaesth 2019;13:208-14.
10. Alsaeid, Mohammed A.; Sayed, Atef M.. Comparison between Position Change after Low-Dose Spinal Anaesthesia and Higher dose with Sitting Position in Elderly Patients: Block Characteristics, Hemodynamic Changes, and Complications. Anaesthesia: Essays and Researches 13(3):p 476-480, Jul–Sep 2019.
11. Sanatkar M, Farhanchi A, Manouchehrian N, Najafi A, Haddadi Sh, Rahmati J, et al. Subarachnoid block with low dose of bupivacaine and sufentanil in patients with coronary artery disease. ARYA Atheroscler 2014; 10(2): 94-9.
12. Jain M, Yadav N, Singh A K (May 03, 2022) Graded Epidural Anaesthesia for Non-cardiac Surgery in the Prone Position in a Patient With Low Ejection Fraction. Cureus 14(5): e24685.
13. Guney I, Argun G. Is Obturator Nerve Block Effective as Spinal Anaesthesia in Preventing Adductor Spasms in General Anaesthesia Without Muscle Relaxants?. Cureus. 2022;14(2):e22365.
14. Sharma D, Singh VP, Agarwal N, Malhotra MK. Obturator Nerve Block in Transurethral Resection of Bladder Tumor: A Comparative Study by two Techniques. Anesth Essays Res. 2017;11(1):101-104.
15. Hermanns, H., Bos, E.M.E., van Zuylen, M.L. et al. The Options for Neuraxial Drug Administration. CNS Drugs 36, 877–896 (2022).
| How to Cite this Article: Sharma V, Aggarwal H, Prakash V, Ahluwalia P. Low Dose Combined Spinal-Epidural (CSE) Anaesthesia with Blocks for Management of A High-Risk Geriatric Patient with Dilated Cardiomyopathy Posted for TURBT. Journal of Anaesthesia and Critical Care Case Reports. September-December 2023; 9(3): 02-05. https://doi.org/10.13107/jaccr.2023.v09.i03.221 |
(Full Text HTML) (Download PDF)