Vol 3 | Issue 2 | May-Aug 2017 | page: 39-40 | Karl Otto Geier.
Authors: Karl Otto Geier [1,2].
[1] Department of Anesthesia, Municipal Hospital Pronto Socorro de Porto, Alegre/RS, Brazil.
[2] Department of Anesthesia and Pain Clinic, São Lucas Hospital da Pontificia Universidade Católica, Porto Alegre/RS, Brazil.
Address of Correspondence
Karl Otto Geier,
Department of Anesthesia and Pain Clinic,
São Lucas Hospital da Pontificia Universidade Católica,
Porto Alegre/RS, Brazil.
E-mail: karlotto42@gmail.com
Lateral femoral cutaneous nerve (LFCN) is a sensory nerve, with its extensive dermatome covering the anterolateral aspect of the thigh. The anatomical knowledge of its extrapelvic courses of the main trunk and its two or more branches immediately below the inguinal ligament (IL) [1-2], explain why the extrapelvic techniques without neural locators (NLs) such as Peripheral Nerve Stimulator (PNS) and Ultrasound (US) devices, are focused on subcutaneous anaesthetic infiltrations in a “fanwise” fashion [3-5], as a field block with volumes up to 15 ml [6]. I would like to present an alternative block without those NL. I usually have performed an intrapelvic approach to block the LFCN as a “single shot” or with cannula for repeated doses. Description of the technique: Local anesthetic (LA) wheal is made. With an angle of 30-40° to the skin immediately below the IL, medial to the anterior superior iliac spine (ASIS), and in a sagittal plane, a set compound by a loss of resistance (LOR) syringe attached to a disposable 20 G needle (3.5 cm to 4.0 cm long) or a 20 G or 22 G intravenous catheter Nipro® (4.2 cm or 5.0 cm long), is advanced toward the great pelvis.
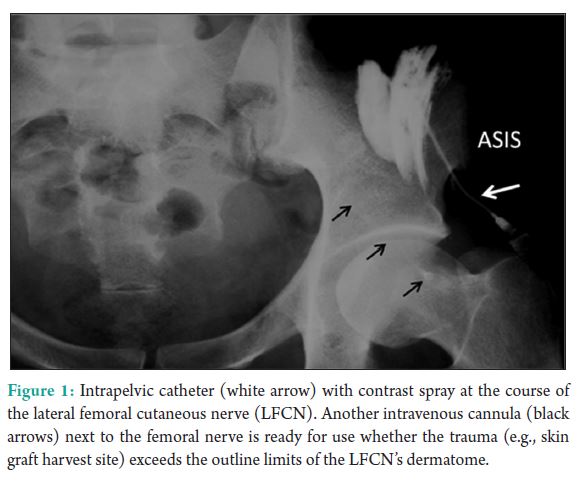
The “end point of the puncture” is determined by two successive resistance losses after has been crossed, the fascia lata and fascia iliaca. With the single needle or venous catheter “in situ,” and its bevel directed slightly lateral, the LOR syringe is replaced by another syringe with 6-7 ml LA and then injected into the iliac fascial compartment. Whether the purpose is to prolong analgesia of wounds, skin grafts, and surgeries (femur osteotomies, osteosynthesis) on the lateral aspect of the thigh, an intravenous catheter is kept in place; the needle is withdraw at the same time where the disposable intravenous catheter is advanced into the iliac fascial compartment and the final LA dose injected. This volume is sufficient to block the LFCN as show at the X-ray (Fig. 1) where the spray (3 ml of LA with 4 ml of Iopamiron® 300) is seen over the course of the LFCN. In my view, short catheters 3.5-5.0 cm long, are ideal for these procedures. Pushing these intravenous catheters toward fascial compartments, hardly result in aleatoryies paths, curls and much less kinks. An extension can be connected to these intravenous catheters offering continuous or intermittent analgesia making its management easy and put them away from the traumatic areas, specially, in skin donor regions at the anterolateral thigh. In places where anesthesiologists have no NL, they can perform this LOR technique. In my opinion, the LOR’s technique is the true art of the peripheral regional anesthesia that not requires the essential technology (PNS and US) to found the peripheral nerves location.
References
1. Doklamyai P, Agthong S, Chentanez V, Huanmanop T, Amarase C, Surunchupakorn P, et al. Anatomy of the lateral cutaneous nerve related to inguinal ligament adjacent bony landmarks and femoral artery. Clin Anat 2008;21:769-74.
2. Dias Filho LC, Valença MM, Guimarães Filho FA, Medeiros RC, Silva RA, Morais MG, et al. Lateral femoral cutaneous neuralgia: An anatomical insight. Clin Anat 2003;16:309-16.
3. Barczewka-Hillel A, Vloka JD. Cutaneous nerve blocks of the lower extremity. In: Hadzic A, editor. Textbook of Regional Anesthesia and Acute Pain Management. New York: McGraw Hill Medical; 2007. p. 558-9.
4. Shannon J, Lang SA, Yip RW, Gerard M. Lateral femoral cutaneous nerve block revisited. A nerve stimulator technique. Reg Anesth 1995;20:100-4.
5. Winnie AP, Ramamurthy S, Durrani Z. The inguinal paravascular technic of lumbar plexus anesthesia: The “3-in-1 block”. Anesth Analg 1973;52:989-96.
6. Meier G, Buettner J. Peripheral Regional Anesthesia. Stuttgart: Thieme; 2006. p. 175-9.
| How to Cite this Article: Geier KO. Lateral femoral cutaneous nerve block with an intravenous catheter. Journal of Anaesthesia and Critical Care Case Reports May-Aug 2017;3(2):39-40. |
