Vol 8 | Issue 1 | January-April 2022 | Page: 14-16 | Luca Pecora, Roberto Procaccini, Danya Falcioni, Sandra Reschini, Luca Farinelli, Diego Tavoletti
DOI: 10.13107/jaccr.2022.v08i01.196
Author: Luca Pecora [1], Roberto Procaccini [2], Danya Falcioni [2], Sandra Reschini [1], Luca Farinelli [2], Diego Tavoletti [1]
[1] Department of Emergency, Anesthesia and Intensive care of Transplantation and Major Surgery, Ospedali Riuniti Ancona, Via Conca, Ancona, Italy.
[2] Department of Clinical and Molecular Science, Marche Polytechnic University, Ancona, Italy.
Address of Correspondence
Dr. Diego Tavoletti,
Department of Emergency, Anesthesia and Intensive care of Transplantation and Major Surgery, Ospedali Riuniti Ancona, Via Conca, Ancona, Italy.
E-mail: diego.tavoletti@libero.it
Abstract
Introduction: Peripheral nerve block is a useful tool for pain relief in trauma patients. Despite this, its use in patients at high risk of developing acute compartment syndrome is still debated. Literature describes that peripheral nerve block causes vasodilatation and an increase in blood flow. However, no reports have evaluated the intracompartmental pressure change after a peripheral nerve block.
Cases presentation: We report five patients with forearm fracture undergoing infraclavicular brachial plexus block. Due to sedation and the unreliability of the clinical signs and symptoms for acute compartment syndrome, intermittent monitoring of intracompartmental pressure was performed before and after the nerve block.
Conclusions: The exact mechanism leading to intracompartmental pressure reduction after brachial plexus block is unclear. Research evaluating the contribution of peripheral nerve block in patients at high risk for acute compartment syndrome are needed.
Keywords: Intracompartmental pressure monitoring, Acute compartment syndrome, Regional anesthesia
Introduction
Acute compartment syndrome (ACS) is a condition in which raised pressure within a closed fascial space reduced capillary perfusion to determine tissue ischemia [1]. ACS is considered a real orthopaedic/traumatology emergency. To avoid a delay in diagnosis, continuous clinical evaluation is necessary. For this reason, the use of peripheral nerve block (PNB) in the setting of patients at high risk for ACS is a hotly debated topic. PNB interrupts the pain transmission pathway, limiting pain perception. This poses a potential risk in the diagnosis of ACS [2, 3].PNB has been previously shown to increase the blood flow in the extremity. Sympathectomy-like effect of the nerve block include a direct effect on the muscularis of the arterial and venous walls as well as increased vessel diameter, blood flow and peripheral resistance reduction [4, 5].However, no one has investigated whether regional anesthesia can cause changes in the intracompartmental pressure of a limb.We report a series of five patients in whom intracompartmental pressure decreased after PNB.
Case Report
Five polytrauma patients with closed radials/ulna shaft fracture and scheduled for open reduction and internal fixation were included in this report.On arrival to emergency room, they were immediately subjected to head to foot survey.Physical examination demonstrated that they were awake, alert and oriented and that they had suffered no neurological injury. Hemodynamic parameters were stable and no respiratory problems were evidenced. After radiographs, three patients showed only forearm fracture and multiple bruises. One patient had pelvic fracture while another patient had vertebral fractures. Initially, patients were evaluated for signs or symptoms of upper limb compartment syndrome, including progressive pain at rest that worsened with passive stretching of the involved muscles as well as paralysis, pallor, paresthesia, hypoesthesia, and pulselessness. All patients reported pain in the arm and other traumatized sites associated with general discomfort. Thus conscious sedation was used to reduce discomfort and widespread pain. In addition, infraclavicular brachial plexus block was performed to abolish pain caused by the fracture. The nerve block was performed using ultrasound guidance and single injection previously described [6]. A total 15 ml of 0.5% levobupivacaine was used for the block.In accordance with the guidelines, an internal protocol stipulated that in obtunded, confused or unco-operative patients with high risk for ACS, direct measurement of intracompartmental pressure should be performed [7].Since the patients were sedated and underwent PNB, the traditional research of clinical signs and symptoms of ACS diagnosis is inaccurate. For this reason, compartment pressure measurements were obtained with a Hand-Held intracompartmental pressure monitor system (Stryker, Kalamazoo, Michigan) in the volar compartment of the forearm. The compartment pressure measurements were performed in two moments: the first immediately before sedation and the PNB, while the second between 90-120 minutes after it.In these cases it was not necessary to perform further measurements, as the open reduction and internal fixation of the radial/ulna fracture took place within 3 hours from the execution of the infraclavicular brachial plexus block.Our protocol predicted that if the surgery was postponed, other measurements would be performed. In addition, an absolute intracompartmental pressure greater than 30 mmHg was considered to be an indication for an emergency fasciotomy [7].
Results
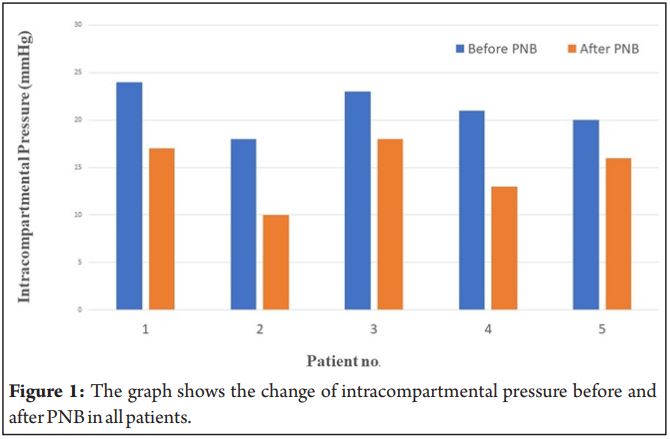
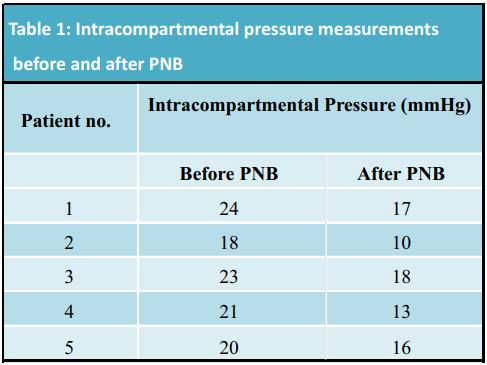
The intracompartment pressure monitoring were successfully performed in all patients studied. Complete infraclavicular brachial plexus block was achieved in all cases and confirmed by the loss of motor and sensory neurological function.There were 4 men and 1 woman with a mean age 45.0 ± 16.3 years, 2weight 73.8 ± 8.1 kg and a body mass index 24.7 ± 2.1 kg/m . Change of the intracompartmental pressure in the ipsilateral forearm are summarized in Table 1. The mean intracompartmental pressure before and after the block was 21.2 ± 2.39 mmHg and 14.8 ± 3.27 mmHg respectively.There was a decrease in intracompartmental pressure after the infraclavicular brachial plexus block (Fig. 1).None of the five patients developed absolute intracompartmental pressure greater than 30 mmHg before the surgery.All infraclavicular brachial plexus block were successful and provided adequate surgical anesthesia.After surgery and during the nerve block, the visual analog scale (VAS) was 0/100 in all patients. The operated extremities showed peripheral pulses, no significant swelling and the forearms remained soft to palpation. When the nerve block was resolved, sensory or motor disabilities were not observed. VAS was less than or equal to 30/100 in all cases and no other signs or symptoms of any ACS were detected.
Discussion
ACS defined as a condition in which the perfusion of the tissue within a closed inelastic osteofascial compartment is compromised by an elevation of interstitial pressure.There are two pathophysiological hypotheses to explain this syndrome: arteriovenous gradient and ischaemic-riperfusion mechanism.In both theories, there is an increase in compartmental pressure which reduces the capillary venous and arterial blood flow. This leads to a reduction oxygen delivery to the tissues, ischemia, release of inflammatory mediators, edema with subsequent increase in extravascular fluids and pressure [7].Long bone extremity fractures are associated with a risk of developing ACS. In literature, the incidence of compartment syndrome is 3% in forearm diaphyseal fractures [8].Clinical signs and symptoms for ACS are unreliable and can lead to delaying his diagnosis [9, 10].Hence, the reference method for diagnosis of ACS is the intracompartmental pressure monitoring [3].Moreover, the diagnosis of ACS can be especially challenging in obtunded and confused patients (e.g traumatic brain injury, sedation), in whom clinical signs may be impossible to elicit. Direct measurement of intracompartmental pressure is indicated in those cases [7].The use of PNB in patients at risk of ACS is a highly controversial topic discussed. Controversy exists concerning the potential of PNB to delay the diagnosis of ACS. Randomized controlled trials comparing outcome after different anesthesia management in patients at risk of ACS have not been performed. Clinical practice is based only on case reports, retrospective case series, recommendations, reviews and currently there is no uniform opinion on the role of PNB in patients at risk of ACS [7].Driscoll et al. analysed 28 case reports and 6 research paper and concluded that in some cases, regional anesthesia or opioid-based, patient-controlled analgesia masked ACS symptoms. However, in most cases where regional anesthesia was documented to delay the diagnosis of ACS, the regional anesthesia technique used was epidural block [11].Some authors have noted that ischemic pain is different from nociceptive or neuropatic pain, and it should not masked when using PNB [12], while this was done using epidural block [11].The explanation is that ischemic pain most likely has a sympathetic component [13]. The ischemic pain related to ACS may be masked with a sympathetic block such as epidural block but not with a PNB, which blocks some sympathetic fibers.In this study, since the patients were sedated and underwent PNB, the traditional research of clinical signs and symptoms of ACS diagnosis is inaccurate. We used an intracompartmental pressure monitor system to quantify any pressure changes in the volar compartment of the ipsilateral forearm after an infraclavicular brachial plexus block. We have observed that an infraclavicular brachial plexus block causes a decrease in compartmental pressure 90-120 minutes after the nerve block.To our knowledge, this study is the first to obser ve an intracomparmental pressure reduction after regional anesthesia.When the pressure inside the compartment increases, the elasticity of the compartment decreases [14]. The nerve conduction block, following regional anesthesia, could lead to reduction in muscle tone and consequently increase the distensibility of the system. In this way the pressure increase in the compartment was counteracted or even reduced. Furthermore, it is commonly accepted that regional anesthesia has a beneficial influence on perfusion and microcirculation [5]. The blockade of sympathetic nerve fibers conduction, due to brachial plexus block, produce arterial and venous dilatation, resistance index reduction, an increase of the blood flow in brachial artery and enhancement in tissue oxygen saturation [4, 5]. These two aspects could oppose to the development of the vicious circle caused by the increase in intracompartmental pressure: compressive closure of the venules, arteriolar compression and tissue ischemia. In this way, tissue edema due to both venous compression and inflammation secondary to ischemia is avoided. The mechanism that led to this result is unknown and this was the only plausible explanation.
Conclusions
Research is required to clarify the impact of PNB on patients at high risk of developing ACS and on the variation in intracompartmental pressure.The available data is limited, and prudent use of regional anesthesia in high risk patient for ACS should be combined with clinical judgment and careful vigilance.
References
1. Morin RJ, Swan KG, Tan V. Acute forearm compartment syndrome secondary to local arterial injury after penetrating trauma. J Trauma. 2009;66:989-93.
2. Vadhanan P, Tripaty DK, Adinarayanan S. Physiollogical and pharmacologic aspects of peripheral nerve blocks. J Anaesthesiol Clin Pharmacol. 2015;31(3):384–93.
3. Klucka J, Stourac P, Stouracova A, Masek M, Repko M. Compartment syndrome and regional anaesthesia: Critical review. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 2017;161(3):242–51.
4. Li J, Karmakar MK, Li X, Kwok WH, Ngan Kee WD. Regional hemodynamic changes after an axillary brachial plexus block: a pulsed-wave Doppler ultrasound study. Reg Anesth Pain Med. 2012;37:111-8.
5. Bosselmann T, Kolbenschlag J, Goertz O, Zahn P, Prantl L, Lehnhardt M, et al. Improvement of Superficial and Deep Cutaneous Microcirculation Due to Axillary Plexus Anesthesia Impaired by Smoking. J Clin Med. 2021;10(10):2114.
6. Fredrickson MJ, Wolstencroft P, Kejriwal R, Yoon A, Boland M, Chinchanwala S. Single versus triple injection ultrasound-guided infraclavicular block: confirmation of the effectiveness of the single injection technique. Anesth Analg. 2010;111:1325-27.
7. Nathanson MH, Harrop-Griffiths W, Aldington DJ, Forward D, Mannion S, Kinnear-Mellor RGM, et al. Regional analgesia for lower leg trauma and the risk of acute compartment syndrome: Guideline from the Association of Anaesthetists. Anaesthesia. 2021.
8. Duckworth AD, McQueen MM. The diagnosis of acute compartment syndrome: a critical analysis review. JBJS Rev. 2017;5(12):e1.
9. Mannion S, Capdevila X. Acute compartment syndrome and the role of regional anesthesia. Int. Anesthesiol Clin. 2010;48(4):85-105.
10. Ulmer T. The clinical diagnosis of compartment syndrome of the lower leg: are clinical findings predictive of the disorder? J Orthop Trauma. 2002;16(8):572-7.
11. Driscoll EB, Maleki AH, Jahromi L, Nelson Hermecz B, Nelson LE, Vetter IL, et al. Regional anesthesia or patient-controlled analgesia and compartment syndrome in orthopaedic surgical procedures: a systemic review. Local Reg Anest. 2016;9:65–81.
12. Kucera TJ, Boezaart AP. Regional anesthesia does not consistently block ischemic pain: two further cases and a review of the literature. Pain Med. 2014;15(2):316–19.
13. Frolich MA, Deshpande H, Ness T, Deutsch G. Quantitative changes in regional cerebral blood flow induced by cold, heat and ischemic pain: a continuous arterial spin labeling study. Anesthesiology. 2012;117:857–67.
14. Sellei RM, Warkotsch U, Kobbe, Weber CD, Reinhardt N, De La Fuente M, et al. Non-invasive and reliable assessment of compartment elasticity by pressure related ultrasound: An in-vitro study. Injury. 2021;52(4):724-30.
| How to Cite this Article: Pecora L, Procaccini R, Falcioni D, Reschini S, Farinelli L, Tavoletti D | Intracompartmental Pressure Change After an Infraclavicular Brachial Plexus Block: A Case Series | Journal of Anaesthesia and Critical Care Case Reports | January-April 2022; 8(1): 14-16. |