Vol 4 | Issue 2 | May-Aug 2018 | page: 4-6 | Shiv Kumar Singh
Authors: Dr. Shiv Kumar Singh [1]
[1] Royal Liverpool University Hospitals Prescot Street Liverpool L7 8XP.
Address of Correspondence
Dr. Shiv Kumar Singh,
Royal Liverpool University Hospitals
Prescot Street Liverpool L7 8XP.
Email: shvkmrsngh@aol.co
Improving safety and quality in regional anesthesia: An innovative app for Indian national regional anesthesia audit database, regional anesthesia database App
Introduction
Regular audit of our own practice has shown to improve quality and safety. Practitioners across the world are able to do it at individual levels but are unable to benchmark it due to unavailability of national or international data. Regional anesthesia has seen an exponential growth in the recent years [1]. In the enthusiasm, many are adopting the newer techniques without appropriate training. Do they know, how well they are doing?, Do they know, they are not causing any harm, and do they know, they are up to standards? In the end, we are all accountable for the service we provide to our patients, surgeons, and institutions [2]. Audits are contractual requirement across many institutions and medical boards around the world. Many anesthetists are quite aware of the audit requirements in their practice but rarely have the time and resources. Moreover, there are significant hurdles and difficulty in establishing clinical audits in real-world practice [7, 8].
Barriers
Paper and web-based data entry may not be the best solution as it is labor intensive and prone to errors, and webbased entry require login which leads to poor participation. Clinicians tend to lose interest very quickly as these methods do not often provide real-time feedback on quality of care and safety. Despite huge number of cases done under purely regional anesthesia techniques, anesthetists from the developing nations rarely do audits and provide data of the real-world medical practice [3]. Electronic medical records and national databases do not exist in many nations and are still fairly far off in the future. At a national level, we need to understand the current practice and outcomes of regional anesthesia to individualize the guidelines and provide support to regional anesthesia enthusiasts. The role of national audit databases (NADs) and registries is well established in quality improvement but rarely exist [4,5]. Even in the low- and middle-income countries, most clinicians use smartphones and with the extensive network availability, are continuously connected. We supported an innovative mobile app (regional anesthesia database [RAD] app and database) developed by one of our members that not only improves audit participation but also provides data from remote geographical locations and enables individual practitioners to develop insight into their own practice that can be compared and benchmarked to improve quality and safety. The mobile app has other features that can provide continuous professional development (CPD) on the go, guidelines, and education at fingertips.
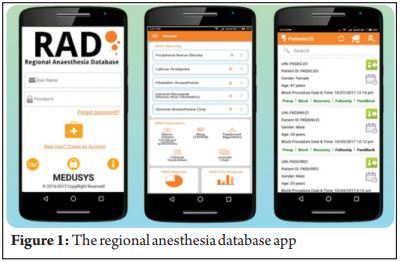
The RAD App
This database project aims to facilitate the collection of consistent quality assurance data to enable current and future benchmarking in regional anesthesia practice across all countries. This large database with enhanced practitioner participation can provide valuable insight into clinical patterns and outcomes along with epidemiological data regarding regional anesthesia. The RAD prospectively collects, collates, and analyses a standardized, nationally agreed peripheral nerve block dataset from all registered users to update benchmark standards of care and provide a powerful quality improvement tool. An iOS and Android-based app along with web interface with built-in analytics were commercially released in July 2017 in India. Individual practitioners and departments obtained license through secure process and user agreements. Data entry involves complete perioperative data entered on smartphone/tablet/web access prospectively at the patient bedside. The mobile app is also enabled for offline data entries and all the data are synced to a secured server. Quality data are ensured by data collection at point of care and several issues identified with paper and web-based registries are addressed.
Safety and Privacy Features
Safety features are inbuilt in the architecture with privacy by design approach (PBD) to comply with most of the health privacy data protection principles in many countries. The database environment has tight monitoring controls along with HIPAA compliance features to assure patient and user privacy is kept secure. The dedicated servers are located in a secure data center in Phoenix, Arizona. It has 100 Mbps bandwidth and in a quakeproof facility. The backup is being taken in a separate HDD in another server in same facility. It is a quad core Xeon processor, 3.5 GHz, 256 GB SSD, 16 GB RAM, Windows Server 2012, MsSql 2012, and 1GBPS LAN.
Protecting Patient Identifiable Data (PID) and Confidentiality
The system generates a unique identifier number for each patient record and will be used for patient follow-up. PID is not recorded or stored in the database. The hospital and user information are encrypted and obfuscated. Only collated results are available for national database, and raw data are not available for any other person apart from the user and database administrator.
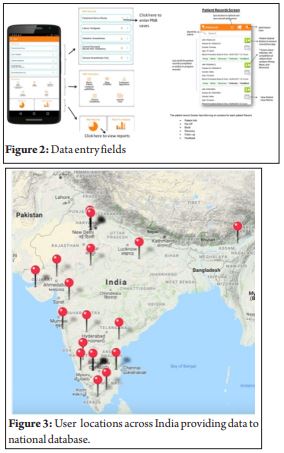
Data entry
There are five data fields to be completed for a complete analysis with some mandatory fields within each dataset. The data entry is made user-friendly with smart entry system to minimize the burden. The three data sets that are mandatorily required for analysis are as follows: Pre-operative details, peripheral nerve block procedural details, and immediate postoperative/recovery data. Patient followup and feedback may not be possible all the time and are kept optional. Data analysis is automated, continuous, and real time with basic descriptive statistics. Filters can be applied in the results section to obtain specific information. Individual results can be compared with national benchmark.
End user Responsibility for Using the Database
Despite the fact that PID protected and confidentiality is maintained, end users have certain responsibilities such as obtaining ethics committee approval/IRB approval, patient consent if required, and data privacy agreement. These are important, especially if individuals are going to present their data at conferences or wish to publish their data. User agreement involves liability clause, data completeness, and entering data accurately and honestly.
Barriers and Solutions
There are several barriers in conducting clinical audits in the real world and can be classified under five main headings. These are lack of resources, lack of expertise or advice in project design and analysis, problems between groups and group members, and lack of an overall plan for audit and organizational impediments [6, 7].
Data Entry at Fingertips
With the use of smartphones, this mobile app (RAD)-based data entry with smart entry features requires minimal effort to contribute patient data to the central database. The immediate real-time feedback through comparative reports is seen as the greatest benefit unlike paper-based or web-based systems.
Applications and Advantages of the Database
This national database will be useful in identifying practice patterns and outcomes. The “real-world” regional anesthesia practice environment from rural health setups to corporate structured metropolitan hospitals can be a great source of information on actual effectiveness of different kinds and techniques of peripheral nerve blocks. It will help organizations to develop national guidelines based on local practice and resources. A large database will help in identifying incidence of complications and associated risk factors. With the help of real-time feedback, anesthetists can identify these flagged risk factors with a potential to reduce complications. Individual practitioners can continually improve care by measuring their outcomes with standards and national trend. From our initial feedback from a small group of users of this RAD app, a number of profound professional benefits have been identified in individual practitioners with improved professional satisfaction, clinical knowledge, and implementing safe clinical practice (user/practitioner feedback). For example, the data entry on safety features including availability of resuscitation equipment and intralipids while doing block and time-out/correct side check has resulted in implementation of measures like buying their own stock of intralipids has resulted in safe and confident anesthetists in the community. The big data in clinical anesthesia have infinite opportunities. Clinical registry databases are considered as new gold standard and are becoming increasingly accepted by both scientific and practitioner communities [9]. It can teach us something we did not know with general advancement of our clinical understanding to increasing scientific knowledge for better therapies for our patients. There is a growing concern among hospitals about accreditation by quality assurance boards such as National Accreditation Board for Hospitals and Healthcare Providers in India since 2007 that requires many measure including clinical audit. However, there is general lack of awareness and lack of resources. This Indian database will provide valuable insight into practice and outcomes of Regional Anaesthesia in India. This innovation will improve audit participation, provide real-world data to national database, and has potential to improve safety and quality in regional anesthesia practice.
Limitations
There are of course several limitations in such e-NAD. The app and database may not be adopted by every clinicians interested in the project. This is a commercial project and utilizes subscription fees from users. This database is entirely based on clinician’s faith on their own quality improvement and integrity; no external validation has been applied yet. A further limitation is of underreporting of complications and failure rates. There is also fear of data sharing and data security.
Future Directions
We intend to setup a clinical registry committee that will comprise members who can institute governance to improve the integrity of the database. Other national databases that are under development are on labor analgesia, obstetrics anesthesia, and non-obstetrics central neuraxial blocks. Many of the benefits of this audit and database are unknown to many practitioners who look at data entry as a boring task with minimal incentive. We intend to use developing technologies to minimize the effort and increase accuracy in data entry. We are developing CPD on the go and journal search initiatives in the app to help anesthetists to be up to date and provide the best care and safe care irrespective of their geographical locations. The next initiative is to develop AI programs and advanced analytics built into the database.
Conclusions
The RAD app and NAD have shown that benchmarking is possible and individual practitioners irrespective of their geographical locations, availability of resources, and other infrastructural limitations can improve the quality of their practice. Using app-based audit data, practitioner participation is enhanced by removing the barriers of conducting a clinical audit in real-life practice. As the national database grows, so will our ability to explore and identify factors that can influence patient outcomes supporting our aim to provide safe anesthesia that enables safe surgery. It will empower and encourage anesthetists across the developing nations to provide data for the nation’s best interest. Going forward, the strength of the The Anaesthetist Society (TAS) NAD will be improved by members taking time out of busy schedules to enter data as fully as is possible. We encourage our members not only to enter their data but also to reflect on analyses of their outcomes. The results of peripheral nerve blocks can assist in providing a national benchmark. Meanwhile, work is in progress to develop the clinical registry committee and website advanced analytics and AI to improve this important function of our audit.
References
- Neal JM, Brull R, Chan VW, Grant SA, Horn JL, Liu SS, et al. The ASRA evidence-based medicine assessment of ultrasound-guided regional anesthesia and pain medicine: Executive summary. Reg Anesth Pain Med 2010;35:S1-9.
- Fisher ES, Shortell SM. Accountable care organizations: Accountable for what, to whom, and how. JAMA 2010;304:1715-6.
- Singh MM, Devi R. Clinical audit: More of a dream than a reality in india. BMJ 2014;348:g2514.
- David SM. What about a national clinical audit results database? BMJ 2014;348:g1303.
- Sites BD, Barrington MJ, Davis M. Using an international clinical registry of regional anesthesia to identify targets for quality improvement. Reg Anesth Pain Med 2014;39:487-95.
- Johnston G, Crombie IK, Davies HT, Alder EM, Millard A. Reviewing audit: Barriers and facilitating factors for effective clinical audit. Qual Health Care 2000;9:23-36.
- Robinson S. Audit in the therapy professions: Some constraints on progress. Qual Health Care 1996;5:206-14.
- Miles A, Bentley P, Polychronis A, Price N, Grey J. Clinical audit in the national health service: Fact or fiction? J Eval Clin Pract 1996;2:29-35.
- Nolan M, Scott G. Audit: An exploration of some tensions and paradoxical expectations. J Adv Nurs 1993;18:759-66.
- Trotter JP. Patient registries: A new gold standard for “real world” research. Ochsner J 2002;4:211-4.
| How to Cite this Article : Singh S K. Improving safety and quality in regional anesthesia: An innovative app for Indian national regional anesthesia audit database, regional anesthesia database App. Journal of Anaesthesia and Critical Care Case Reports May-Aug 2018; 4(2):4-6. |