Vol 3 | Issue 1 | Jan-Apr 2017 | page: 5-7 | Yogen Bhatt, Girija Yadav, Smitha Rao.
Authors: Yogen Bhatt [1], Girija Yadav [2], Smitha Rao [3]
[1] Director, Anaesthesia Basic and Critical Care Plus Co.
[2] Consultant Anaesthesiotogist, NAMAH Hospital & Kapadia Multispecialty Hospital, Mumbai.
[3] Consultant Anaesthesiologist, Shalyak Hospital & Dr MASRANI’s Hospital, Mumbai
Address of Correspondence
Dr. Y Bhatt
1702, Tower -3, Rustomjee Ozone, Vasari Hill Rd,
Behind Mtnl. Goregaon West. Mumbai 62.
Email: yogenbhatt1@gmail.com
Abstract
Introduction: A healthy adult male posted for a minor perianal procedure had an unprecedented circulatory collapse during surgery where hydrogen peroxide was used for instillation. At the onset of the event, we could auscultate a pan cardiac murmur, loudest ever heard which disappeared in about a minute while the phase of deterioration continued for about 3-4 minutes followed by dramatic improvement. After ruling out other causes, the most likely diagnosis was an embolic phenomenon. Venous air embolism is a well known entity and hydrogen peroxide as an etiology has been reported in several cases but the numbers are not in league with its rampant use in medical field. Thus, we wish to report the same along with a brief on its management.
Keywords: Embolism, Hydrogen Peroxide, Circulatory collapse.
Introduction
Venous Air Embolism (VAE) is the entrainment of air (or exogenously delivered gas) from an open operative field or communication with environment into the venous or arterial vasculature producing systemic effects [1] which are catastrophic with high mortality.
It may arise from a surgical procedure where the operative site is above the level of heart such as: sitting neurosurgical procedure, obstetric procedure and orthopedic surgeries. VAE can also arise from iatrogenic creation of pressure gradient that facilitates entry of air into circulation such as during insertion of central venous catheter or from mechanical insufflations or pressure infusion such as laparoscopic surgeries and gastrointestinal endoscopies. Last but not the least, introduction of exogenous gas releasing substance may also cause VAE.
Hydrogen peroxide (H2O2) is indicated at oncentrations of up to 6% for disinfection of minor cuts, wounds and skin ulcers. It rapidly decomposes to water and oxygen, therefore is often considered to be a harmless and user‐friendly antiseptic and cleansing agent. However, since even 1 ml of 3% H2O2 produces 9.8 ml oxygen, serious complications can arise if this is liberated in the vascular bed. Our surgery was not amongst one of those counted to be as high risk for VAE, and H2O2 has been implicated in some cases of life threatening or fatal gas embolism wherein cardiorespiratory collapse occurred within seconds to minutes of instillation of hydrogen peroxide for wound irrigation or when used to soak swabs for wound packing [2,3,4].
Case Report
58 yr old male weighing 70 kg, well maintained on diet control with normal lab work up and electrocardiogram (ECG) was posted for fistula-in-ano surgery.
After confirming nil per oral status and consent, haemo glucose test (HgT) of 106mg/dl, standard monitors for saturation of oxygen (SpO2), pulse rate, ECG and non invasive blood pressure (NIBP) were attached.
After pre-oxygenation and premedication with glycopyrolate 0.2 mg, midazolam 1.5 mg and fentanyl 100µg , general anaesthesia (GA) was induced with propofol 100 mg and atracurium 40 mg. Proseal laryngeal mask airway (LMA) no.5 was inserted, checked and fixed. Mechanical ventilation was maintained with 50% nitrous oxide (N2O) in oxygen and 1% isoflurane. After confirming adequate ventilation, oxygenation and comfortable airway pressures, lithotomy position was given after which all parameters were re-checked and found to be stable.
Surgery was started after giving 15-20° trendlenburg position. Intraoperatively, a mixture of methylene blue and hydrogen peroxide was used to assess extent and inner opening of the fistula. Suddenly at 35 mins, as the surgeon was instilling the mixture with a 20cc syringe into the fistula after partial dissection of the external opening to locate multiple internal openings, the pulse waveform on the monitor disappeared .The SpO2 probe was checked and applied on another finger but no waveform was appreciable. The radial artery pulsation also ceased to be felt bilaterally, however the monitor showed normal sinus rhythm going up to heart rate (HR) of 120, SpO2 100% (only numerical value) and NIBP 124/82 mm of Hg. Bilateral axillary artery compression due to faulty positioning was checked for while the next reading showed a precipitous fall in NIBP to 50 systolic with gradually dropping trend of SpO2 to 45 and increasing tachycardia of 140. Unfortunately, end tidal carbondioxide (ET CO2) monitor was unavailable. On auscultation, there was a harsh murmur heard throughout the cardiac cycle with normal respiratory sounds.
All agents were turned off and 100% oxygen (O2) was started. IV fluid bolus and inj. mephentermine in boluses of 6 mg (with no response) was given while LMA was replaced by a more secure 8 no.ETT. With impending cardiorespiratory collapse, noradrenaline infusion was started. ETCO2 monitor & defibrillator were arranged while right internal jugular vein cannulation site was being prepared when suddenly all parameters started to stabilize at 3-4 minutes of the event.
The SpO2 improved over just a few seconds and reached about 95% in no time. The ECG had shown sinus rhythm throughout.
A 12 lead ECG showed absolutely normal rhythm with rate of 86, repeat HgT was found to be 100.There were no rashes on his body or any flushing or perspiration. The bladder was catheterised and urine appearance was normal. Later, it was found that the surgeon had instilled about 30 ml of hydrogen peroxide at fistula site.
As all parameters remained stable along with normal ETCO2 reading of 32-34 mm Hg with good waveform, isoflurane was turned on and surgery resumed (withholding any further instillation of peroxide) and completed in 15 minutes. 200 mg hydrocortisone and 100ml 20% manittol were given to take care of any Hypoxic Cerebral edema. IV paracetamol 1g and local infiltration with 10cc 0.25% bupivacaine was carried out for post op analgesia.
At stable vital parameters and attempts to breathe, reversal was carried out with incremental doses of neostigmine with glycopyrrolate and patient was extubated smoothly.
2 hrs post surgery, patient was comfortable with stable vitals and no neurodeficit and on direct questioning refused any awareness during procedure.
Bilateral lower limb Doppler study carried to rule out any deep vein thrombosis (DVT) or plaques was normal and so was the resting 2D Echo. Cardiac enzymes were not elevated.
Patient recovered completely and was discharged in 3 days.
Discussion
The danger of injecting H2O2 under pressure in closed or semi‐closed cavities [5,6,7] is that it may force H2O2 into blood vessels, rapidly producing critical amounts of gaseous oxygen. In our case, 30 ml of 3% H2O2 was probably sufficient to trigger a venous gaseous embolism, since it was injected under pressure into a semi‐closed space which is known to have extensive venous drainage.
Presentation of VAE varies according to the nature, volume and speed of air entrainment into the circulation. Smaller amount does not cause any clinical manifestations as it gets absorbed from circulation. Moderate amount of air causes pulmonary vascular injury leading to pulmonary hypertension and permeability pulmonary oedema [8], whereas a larger bolus will cause right ventricular flow obstruction.
Slow infusion of air (0.01–2.00 ml/kg/min) passes through the right side of the heart, and occludes the pulmonary circulation causing a progressive increase in central venous pressure (CVP) and an increase in pulmonary arterial pressure (PAP). In contrast, injection of a bolus air (25–200 ml; 1–13 ml.kg/min) immediately occludes the right side of the heart, increases CVP, decreases PAP, and causes significant hemodynamic instability [9, 10].
In up to 35% of patients, due to the presence of patent foramen ovale the air passes from right side to the left side of the heart leading to systemic air embolization termed as paradoxical embolism [11] causing cerebral and myocardial ischemia .The fatal amount of air in human is reported to be either 200 and 300 ml bolus or 3-5 ml/kg. [12].
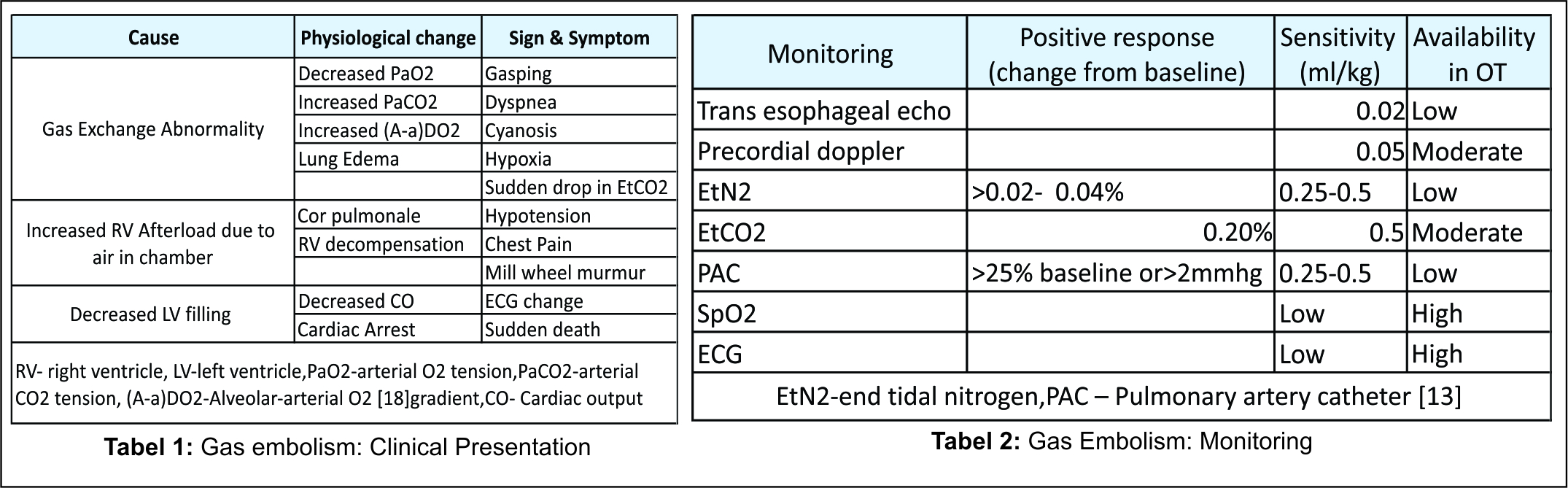
The Clinical Presentation is summarised in table 1.
High index of suspicion in high risk cases is the corner stone for diagnosis of VAE and should be considered when unexplained hypotension or sudden decrease in end-tidal CO2 level occurs intraoperatively in high risk cases.
The available monitoring with its sensitivity is tabulated below in Table 2
Additionally,Transcranial Doppler [14] may pick up air bubbles, Ventilation Perfusion scan would show a perfusion defect which gets resolved rapidly usually within 24 hours. CT chest will show air in central venous system, ventricles, pulmonary artery or pneumothorax. CT brain may show intravascular air with or without infarction [15].
The management is summarised in Table 3
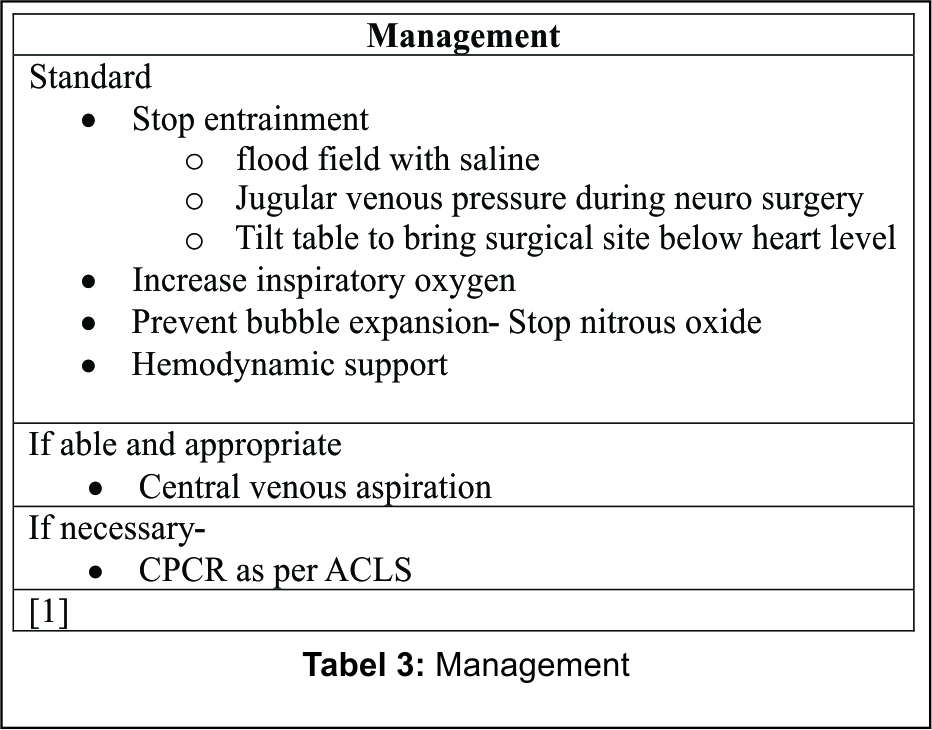
Since H2O2 might be partially forced into the vascular bed at the time of injection and before it vaporizes, flooding the wound with saline will not prevent the risk of gas entrapment within the capillaries.
The circulating gas is eliminated by molecular diffusion directly across the arteriolar wall into the alveolar spaces, depending on partial pressure difference between the capillaries and the alveoli. In the case of oxygen bubbles created by H2O2 within the pulmonary circulation, if 100% oxygen is applied to the alveolar space, the partial pressure difference theoretically falls to zero, preventing any excretion. Most patients treated with 100% oxygen have recovered without long‐term complications after oxygen emboli; there are also other mechanisms of elimination such as metabolism and absorption, mainly in peripheral tissues. Ventilating the lungs with 100% oxygen can still be considered necessary, since the cause of the hypoxia and fall in ETCO2 may not always be clear initially.
VAE should be differentiated from acute coronary syndrome, cardiogenic shock, anaphylactic shock, cerebrovascular accidents, and pulmonary thromboembolism. As in our case, we ruled out other diagnoses with a normal ECG, cardiac enzymes and 2D echo and lower limb Doppler studies. We could have also done neuroimaging and CT Pulmonary angiography, however as the patient recovered fully with no sequelae it was not performed.
Conclusion
Our surgery was not amongst one of those counted to be as high risk for VAE as has been implicated for H2O2 in some cases. However, as H2O2 was used in a huge quantity, we believe it to be the cause of the embolic event.
VAE from H2O2 is an established entity and we need to restrict its use in large quantities especially for pressurised lavage of enclosed space with known good vascularity. In case it is being used, we must be equipped to handle life threatening events with necessary infrastructure. It will be a good measure to use diluted H2O2 in limited quantities if deemed necessary.
References
1. Mirski MA, Lele AV, Lunei Fitzsimmons, Toung TJ. Diagnosis andtreatment of vascular air embolism. Anesthesiology 2007;106:164–77. [PubMed: 17197859]
2. Haller G, Faltin-Traub E, Faltin D, et al. Oxygen embolism after hydrogen peroxide irrigation of a vulvar abscess. Br J Anaesth 2002;88:597–9[Pubmed :12066743]
3. Dubey PK, Singh AK. Venous oxygen embolism due to hydrogen peroxide irrigation during posterior fossa surgery. J Neurosurg Anesthesiol 2000;12:54–6[Pubmed : 10636622]
4. Chhabra R, Pathak A, Ray P. Fatal posterior fossa pneumocephalus due to hydrogen peroxide irrigation of lumbar wound. Br J Neurosurg. 2000;14(6):549-51. [Pubmed :11272033]
5. Donati S, Barthelemy A, Boussuges A, Gainier M, et al. Severe air embolism after surgical irrigation with hydrogen peroxide. Presse Med 1999;28:173–5 [Pubmed :10071628]
6. Morikawa H, Mima H, Fugita H, Mishima S. Oxygen embolism due to hydrogen peroxide irrigation during cervical spinal surgery. Can J Anaesth 1995; 42:231–3. [ Pubmed :7743577]
7. Tsai SK, Lee TY, Mok M. Gas embolism produced by hydrogen peroxide irrigation of an anal fistula during anesthesia. Anesthesiology 1985;63:316–7.[Pubmed :4025893]
8. Fitchet A, Fitzpatrick AP. Cerebral venous air embolism causing pulmonary edema mimicking left ventricular failure. BMJ. 1998;16:604–6. [PMCID: PMC1112636] [PubMed: 9518916]
9. Holcomb BW, Loyd JE, Byrd BF, 3rd, Wilsdorf TT, Casey-Cato T, Mason WR, et al. Iatrogenic paradoxical air embolism in pulmonary hypertension. Chest 2001;119:1602–5. [PubMed: 11348976]
10. Toung TJ, Rossberg MI, Hutchins GM. Volume of air in a lethal venous air embolism. Anesthesiology 2001;94:360–1. [PubMed: 11176104]
11. Chen X-C, Tang X-Y, Jiang Y-F, Pan Y-B, Fu C-Z. Sudden cardiovascular collapse caused by carbon dioxide embolism during endoscopic saphenectomy for coronary artery bypass grafting. Chinese Medical Journal 2006;119:345–8 .[Pubmed : 16537035]
12. Lee S, Choi B, Kim J, Park K. Paradoxical air embolism during hepatic resection. British Journal of Anaesthesia 2002; 88:136–8. [Pubmed :11883374]
13. Kim C, Liu J, Kwon J, et al. Venous air embolism during surgery, especially cesarean delivery. J Korean Med Sci. 2008;23:753-61. [Pubmed:18955777]
14. Stendel R, Gramm HJ, Schröder K, Lober C, Brock M. Transcranial doppler ultrasonography as a screening tool for detection of patent foramen ovale before surgery in sitting position. Anesthesiology 2000;93:971–5.
[PubMed: 11020748]
15. Valentino R, Hilbert G, Vargas F, Grison D. Computed tomographic scan of massive cerebral air embolism. Lancet 2003;361:1848. [PubMed:12788570].
| How to Cite this Article: Bhatt Y, Yadav G, Rao S. Hydrogen peroxide causing embolism in perianal surgery. Journal of Anaesthesia and Critical Care Case Reports Jan-Apr 2017; 3(1):5-7. |
