Vol 3 | Issue 2 | May-Aug 2017 | page: 41-42 | Priyanka Rathi, Arati Ghorpade.
Authors: Poonam Ghodki [1], Jyoti Mundavare [1].
[1] Department of Anaesthesiology and Critical Care, Smt. Kashibai Navale Medical College, Pune, Maharashtra, India
Address of Correspondence
Dr. Poonam Ghodki,
Department of Anaesthesiology and Critical Care,
Smt. Kashibai Navale Medical College,
Pune, Maharashtra, India.
E-mail: drpoonamghodki@gmail.com
Introduction
Of the plethora of technical skills that an anesthetist should possess, airway management skills will forever remain cardinal. Successful outcome of anticipated difficult intubation largely depends on proper pre-operative evaluation, assessment, planning, preparation, and finally execution. We hereby present the airway management of an extremely huge hydrocephalus posted for surgery where we employed all the above components.
Pre-operative evaluation and assessment
The patient: 4 months old male baby with head circumference 70 cm (Fig. 1). Weight – 5 kg apparent body weight roughly 2.5 kg, rest was the weight of the head. No other congenital anomaly. There was a tendency of the child to sleep in the lateral position; consequently, largest head diameter was occipitofrontal.

Planning
We calculated the head width at the occipitofrontal line to know the elevation needed beneath the body to make the patient lie supine. This “stacking” amounted to one adult pillow and two blankets (Fig. 2).
Preparation
General anesthesia with an endotracheal tube (ETT) under spontaneous sevoflurane induction was planned. Stacking was done on the operation table. Using materials for creating the “ramp” position is well known in obese patients or in patients suffering from ankylosing spondylitis. The “ramp” literally means an inclined surface, while we used a straight surface to accommodate the body beyond the head. This constitutes the “stacking” position (Fig. 3).

A 3.5 number ETT was straightened with stillete to ease intubation (Fig. 4).

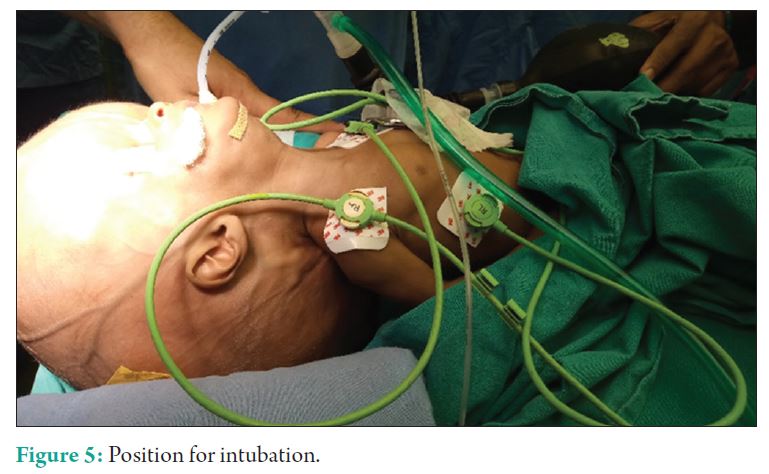
Execution
Patient’s head (occiput) was placed on a thin head ring while the body rested on the stack. The three axis of intubation were aligned in this position. The patient was induced with sevoflurane and fentanyl. Miller blade was used for laryngoscopy and patient was intubated at the first attempt with 3.5 ETT (Fig. 5).
Inference
The importance of dexterity in managing anticipated difficult airway cannot be overstated. This extremely difficult looking airway was made simpler once the most important hurdle was taken care of, i.e., appropriate positioning. The patient, with the help of stacking, could be made supine in such a way that the external auditory meatus and sternum were in a straight line [1]. This ensured alignment of oral, laryngeal, and tracheal axis to aid intubation. Other possible techniques would be intubating in lateral position or with the head hanging and held in assistant’s hand at the edge of the table [2]. These techniques do not guarantee intubation, moreover, their suitability for such huge hydrocephalus is not known.
Conclusion
“If you do not get the BASICS right, things can turn ACIDIC anytime!” One has to concord with the basics of airway
management while planning for anticipated difficult airway scenario. Logistic planning and skilful execution prevent from landing up in an “unable to oxygenate” situation.
Acknowledgement
Straightening of ETT for pediatric patients was originally described by Dr. Raghavendran Kalyansundaram on “The Anaesthetist Society” group discussion. He described intubation through the groove in Miller’s blade; we however barely straightened the ETT and intubated conventionally. Quote used by Dr. Anil Sharma on the “The Anaesthetist Society” group discussion.
References
1. Sunder RA, Haile DT, Farrell PT, Sharma A. Pediatric airway management: Current practices and future directions.
Paediatr Anaesth 2012;22:1008-15.
2. Rajan S, Paul J, Andrews S. Induction and intubation in a Kleeblattschadel syndromic child with posterior cranial
distractors. J Anaesthesiol Clin Pharmacol 2014;30:440-2.
| How to Cite this Article:Ghodki P. Extremely huge hydrocephalus for surgery: Difficult intubation made easy! Journal of Anaesthesia and Critical Care Case Reports May-Aug 2017;3(2):41-42. |
