Vol 5 | Issue 1 | Jan-Aprl 2019 | page: 3-5 | Valluvan Rangasamy, Balachundhar Subramaniam
Authors: Valluvan Rangasamy [1], Balachundhar Subramaniam [1].
[1] Center for Anesthesia Research Excellence, Department of Anesthesia, Critical Care, and Pain Medicine, Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, MA, USA.
Address of Correspondence
Dr. Balachundhar Subramaniam,
Elliot C. “Jeep” Pierce Associate Professor of Anaesthesia, Harvard Medical School, Director, Center for Anesthesia Research Excellence, Beth Israel Deaconess Medical Center, Boston, MA, USA.
E-mail: bsubrama@bidmc.harvard.edu
Evaluation of geriatric physiological reserve – Keeping an ear to the ground
An increasing number of elderly patients presenting for surgery has profound implications for perioperative medicine. Around half of the surgeries, in the United States were done among elderly patients [1]. Unique physiological changes result in multisystem decline and increase their vulnerability for complications. Frailty expresses this phenomenon and has been considered as a state of decreased physiological reserve and resistance to stressors. Although more common with age, frailty is a distinct concept of biological rather than chronological age [2]. Moreover, the underlying mechanisms of frailty are different from aging. Hence, frailty could explain the observed variations in clinical outcomes that cannot be explained by chronological age alone.
Substantial stressor like surgery in frail patients could result in a disproportionate change from independent to dependent, mobile to immobile, stable posture to frequent falls, or lucid to delirious state. Emerging evidence demonstrates increased perioperative complications associated with frailty and incorporating frailty assessment has shown to improve prognostication of existing risk stratification tools [3]. The two widely accepted models of frailty include a phenotypic construct and a deficit accumulation model. However, there is no clear consensus regarding a standard method to assess frailty.
Recent evidence suggests autonomic dysfunction could possibly be the underlying mechanism behind frailty and perioperative complications [4]. Being mainly regulated by the autonomic nervous system, blood pressure (BP) variability is significantly affected by autonomic dysfunction. The relationship between BP variability (beat to beat change) independent of the individual BP numbers on perioperative adverse outcomes has gained increased interest recently [5, 6]. Various methods were used to study BP variability. However, these methods do not describe the temporal dynamics of the BP waveform.
The importance of temporal structure can be explained by the following two sequences: A = {1232123212321} and B = {1111222222333} [5, 7]. Both have the same variability, measured by the range and standard deviation, but completely different structures. Sequence A defines a triangular wave whereas sequence B is a step function. With advanced technology to capture beat-to-beat BP values and computational methods, the temporal dynamics of the BP waveform could be analyzed easily. BP complexity similar to frailty reflects the physiologic reserve and adaptive responsiveness of the system to stress. Recent evidence reports a significantly lower BP complexity in patients with adverse outcomes [5]. Furthermore, BP complexity indices were found to correlate with standard risk prediction scores [8]. Hence, frailty and complexity could possibly be a surrogate of an individual’s physiological reserve.
The 2010 National Confidential Enquiry into Patient Outcome and Death from the UK found that frailty was not included in the risk assessment of elderly patients. They recommended to include frailty in perioperative risk assessment [9]. Despite recommendations from major organizations (American Chemical Society, Anesthetic Groups, and Association of Anaesthetists of Great Britain and Ireland), frailty is rarely used in routine perioperative care. Multiple methods are used to assess frailty. Their limitations such as time consumption need for specialized training or evaluation and difficulty with emergency surgeries has prohibited their widespread pre-operative use. A tool based on collected patient data could be promising for frailty assessment. Frailty index constructed based on BP complexity and routinely collected clinical data might be reassuring. An index derived in this manner is more likely to be adopted and maintained in clinical practice.
The frail (aging) brain is associated with characteristic age-related changes. Disproportionately affected hippocampal pyramidal neurons [10] and hyper-responsive microglia [11] are proposed to play a role in the pathophysiology of neurocognitive disorders. Post-operative delirium (POD) and post-operative cognitive dysfunction (POCD) are a growing concern among elderly patients. POD is an acute dysfunction with symptoms including disorientation, impairment of attention and memory. POCD is a persistent cognitive disorder that lasts from a few hours to several days or months. Among multiple contributing factors, chronological age is nonmodifiable whereas frailty, pre-operative cognitive function, and neurocognitive reserve were proposed as modifiable [12]. Evidence from literature supports a temporal association between frailty, cognitive decline, delirium, and dementia [13, 14]. Therefore, identifying and targeting interventions toward at-risk patients could help in preventing adverse outcomes.
Predicting operative risk among elderly patients is challenging due to their discrepancies in health status and inadequacy of assessment tools. Commonly used predictors such as American Society of Anesthesiologists score, Charlson Comorbidity Index, and Lee’s cardiac risk index are either subjective or based on organ systems, and none of them actually account for an individual’s physiological reserve. Despite the widespread use of existing tools, complications in the elderly surgical population remain difficult to predict. Surprisingly, no standard method to assess physiological reserve exists.
We anesthesiologists often fail to recognize frailty in the perioperative setting. Hubbard and Story in their recent review referred frailty as the “elephant in the operating room: Easy to spot but is often ignored” [15]. Furthermore, the subtler forms of neurocognitive disorders (POD and POCD) may often go undetected resulting in increased morbidities in the elderly patients. These disorders often result from an acute insult on a vulnerable patient. Patients with frailty, a validated marker for vulnerability could possibly be at an increased risk for developing these disorders.
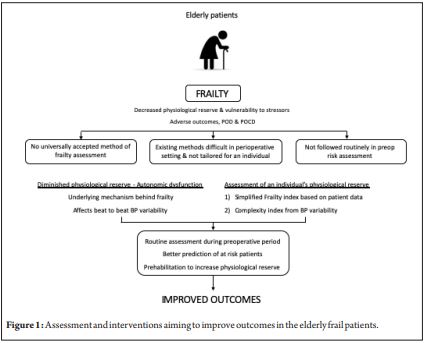
To summarize, the elderly patients are assessed based on their medical conditions alone without accounting for their physiological reserve. Incorporating measurements of an individual’s physiological reserve such as (a) frailty based on easily available pre-operative data or (b) complexity derived from pre-operative BP might provide a means for anesthesiologists to identify high-risk patients (Fig. 1). This could be achieved with the help of advancements in health informatics and electronics. With better identification, potential interventions aiming to reduce complications could be accomplished. Prehabilitation is one such intervention which could possibly improve outcomes. It improves the physiological reserve to withstand any stress associated with surgery. A paradigm shift in the pre-operative assessment emphasizing individualized risk is vital and could possibly the future of perioperative medicine.
References
1. Popovic JR. 1999 national hospital discharge survey: Annual summary with detailed diagnosis and procedure data. Vital Health Stat 13 2001;1-5.
2. Anand A, Harley C, Visvanathan A, Shah AS, Cowell J, MacLullich A, et al. The relationship between preoperative frailty and outcomes following transcatheter aortic valve implantation: A systematic review and meta-analysis. Eur Heart J Qual Care Clin Outcomes 2017;3:123-32.
3. Dent E, Kowal P, Hoogendijk EO. Frailty measurement in research and clinical practice: A review. Eur J Intern Med 2016;31:3-10.
4. James LA, Levin MA, Lin HM, Deiner SG. Association of preoperative frailty with intraoperative hemodynamic instability and postoperative mortality. Anesth Analg 2019.
5. Subramaniam B, Khabbaz KR, Heldt T, Lerner AB, Mittleman MA, Davis RB, et al. Blood pressure variability: Can nonlinear dynamics enhance risk assessment during cardiovascular surgery? J Cardiothorac Vasc Anesth 2014;28:392-7.
6. Jinadasa SP, Mueller A, Prasad V, Subramaniam K, Heldt T, Novack V, et al. Blood pressure coefficient of variation and its association with cardiac surgical outcomes. Anesth Analg 2018;127:832-9.
7. Packiasabapathy KS, Subramaniam B. Optimal perioperative blood pressure management. Adv Anesth 2018;36:67-79.
8. Henriques TS, Costa MD, Mathur P, Mathur P, Davis RB, Mittleman MA, et al. Complexity of preoperative blood pressure dynamics: Possible utility in cardiac surgical risk assessment. J Clin Monit Comput 2019;33:31-8.
9. National Confidential Enquiry into Patient Outcome and. Elective and Emergency Surgery in the Elderly: An age old Problem; 2010.
10. Panegyres PK. The contribution of the study of neurodegenerative disorders to the understanding of human memory. QJM 2004;97:555-67.
11. van Gool WA, van de Beek D, Eikelenboom P. Systemic infection and delirium: When cytokines and acetylcholine collide. Lancet 2010;375:773-5.
12. Berger M, Terrando N, Smith SK, Browndyke JN, Newman MF, Mathew JP, et al. Neurocognitive function after cardiac surgery: From phenotypes to mechanisms. Anesthesiology 2018;129:829-51.
13. Eeles EM, White SV, O’Mahony SM, Bayer AJ, Hubbard RE. The impact of frailty and delirium on mortality in older inpatients. Age Ageing 2012;41:412-6.
14. Rogers NT, Steptoe A, Cadar D. Frailty is an independent predictor of incident dementia: Evidence from the english longitudinal study of ageing. Sci Rep 2017;7:15746.
15. Hubbard RE, Story DA. Patient frailty: The elephant in the operating room. Anaesthesia 2014;69 Suppl 1:26-34.
| How to Cite this Article: Rangasamy V, Subramaniam B. Evaluation of geriatric physiological reserve – Keeping an ear to the ground. Journal of Anaesthesia and Critical Care Case Reports Jan-April 2019;5(1):3-5. |

(Full Text HTML) (Download PDF)
.