Vol 10 | Issue 1 | January-April 2024 | Page: 05-07 | Amanda Myles, Sheryl S. Ang
DOI: https://doi.org/10.13107/jaccr.2024.v10.i01.229
Open Access License: CC BY-NC 4.0
Copyright Statement: Copyright © 2024; The Author(s).
Submitted: 07/04/2023; Reviewed: 02/05/2023; Accepted: 21/10/2023; Published: 10/01/2024
Author: Amanda Myles [1], Sheryl S. Ang [1]
[1] Department of Anesthesiology and Perioperative Medicine, Medical College of Georgia at Augusta University, Augusta University Medical Center, GA, USA.
Address of Correspondence
Dr. Amanda Myles,
Department of Anesthesiology and Perioperative Medicine, Medical College of Georgia at Augusta University, Augusta University Medical Center, GA, USA.
E-mail: a33myles@comcast.net
Abstract
Background & Case: A 38-year-old Spanish-speaking, pregnant woman at 26.1 weeks’ gestation with two previous Cesarean sections (C-section) presented with acute respiratory distress syndrome secondary to COVID-19 pneumonia. She was intubated and ventilated, complicated by bilateral pneumothoraces and emphysema requiring bilateral chest tubes and blow holes. She had worsening hypoxic respiratory failure ultimately requiring cannulation for venovenous extracorporeal membrane oxygenation (VV-ECMO). She was started on cefazolin for Methicillin-susceptible Staphylococcus aureus bacteremia. On day three of VV-ECMO, there was non-reassuring fetal heart tone necessitating emergent bedside non-sterile Cesarean section at 27.2 weeks’ gestational age in the surgical intensive care unit. Post-Cesarean section, her respiratory failure improved, and she was decannulated from VV-ECMO 13 days later. This case report highlights that VV-ECMO can be a life-saving treatment option for pregnant women with cardiopulmonary failure who are unresponsive to conventional therapy. Literature describing Caesarean section on VV-ECMO is limited. Specifically, there have been only a handful of case reports of C-sections on patients put on VV-ECMO due to respiratory failure.
Results: The obvious benefit of proceeding with this emergent bedside C-section was to save the fetus. However, this had to be weighed against the risks of hemorrhage in this high-risk patient since she had two previous C-sections and was on a therapeutic heparin drip while on VV-ECMO. Additionally, there is the risk of infection due to having the C-section done in a non-sterile manner, especially in a patient who is bacteremic. This was mitigated by using additional prophylactic antibiotics post-operatively. The patient’s respiratory status improved significantly after the fetus was delivered, likely due to improvements in respiratory mechanics post-partum. The successful outcome of this patient and her baby required the timely coordination of a
multidisciplinary team.
Conclusions: Emergent C-section on a pregnant woman with respiratory failure on VV-ECMO can be life-saving for the fetus and the mother. However, the inherent risks associated with it requires close monitoring of the patient and the fetus in order to determine when this is truly necessary.
Keywords: Acute respiratory distress syndrome, Cesarean-section, COVID-19, Pregnancy, Veno-venous extracorporeal membrane oxygenation
Introduction
Demand for veno-venous extracorporeal membrane oxygenation (VV-ECMO) has increased during the COVID-19 pandemic [1]. VV-ECMO can be a life-saving treatment option for pregnant women with cardiopulmonary failure who are unresponsive to conventional therapy. Overall maternal and fetal survival on ECMO are 80% and 70%, respectively [2]. With VV-ECMO, the blood is drained from the right atrium (RA) and goes through a membrane lung or oxygenator, a gas exchange device that uses a semipermeable membrane to add and remove gases from the blood. This oxygenator is placed sequentially with the normal lungs, reducing the workload on the lungs3. Then, the newly oxygenated blood is returned to the RA, and the newly oxygenated blood added to the native venous blood provides enough systemic oxygen delivery. In hypoxic respiratory failure, VV-ECMO therapy is indicated when the risk of mortality is greater than or equal to 80% [4].
Regarding ECMO in pregnancy, a 2020 systematic review in the Journal of the American Heart Association reviewed 358 women [5]. This review found that the most common indication for ECMO was acute respiratory distress syndrome, as seen in 49.4% of the women. The aggregate maternal survival at 30 days was 75.4% and at 1 year was 74.3%. These reports of survival in pregnancy and in the postpartum periods are relatively high. The most common maternal complication was mild to moderate bleeding which was seen in only 18.4% of the women as well as severe bleeding necessitating surgical intervention in 13.4% of the women. There were 68 reported fetal outcomes with a survival rate of 64.7%. Additionally, preterm delivery was seen in about half of the of the fetuses and there were 19 (27.8%) neonatal intensive care unit admissions.
Additionally, a recent 2022 multicentre, retrospective cohort was completed on maternal and fetal short and long term outcomes of pregnant women on ECMO for severe respiratory distress syndrome [6]. This cohort showed no difference in maternal outcomes. Results show that continuation of the pregnancy on ECMO improves prematurity-related morbidity while bringing a significant risk of fetal death.
By the end of July 2022, 225,656 cases of COVID-19 in pregnant women were reported in the United States, including 34,693 hospitalized cases [5]. Literature describing Caesarean section (C-section) on VV-ECMO is limited. Specifically, there have been only a handful of case reports of C-sections on patients put on VV-ECMO due to respiratory failure secondary to H1N1 flu [8], hemoptysis [9], or COVID-19 [10].
Case Description:
A 38-year-old Spanish pregnant woman at 26.1 weeks’ gestation with two previous C-sections presented (day one) with acute respiratory distress syndrome secondary to COVID-19 pneumonia. She had no significant past medical history.
She initially required high-flow nasal cannula and was started on dexamethasone for fetal lung maturity and twice-a-day fetal monitoring. The next day, she developed worsening acute hypoxic respiratory failure requiring intubation and mechanical ventilation. This was complicated by bilateral pneumothoraces and subcutaneous emphysema which required bilateral chest tubes and blow holes. When patient was transferred to the intensive care unit (ICU), continuous fetal heart rate monitoring was initiated.
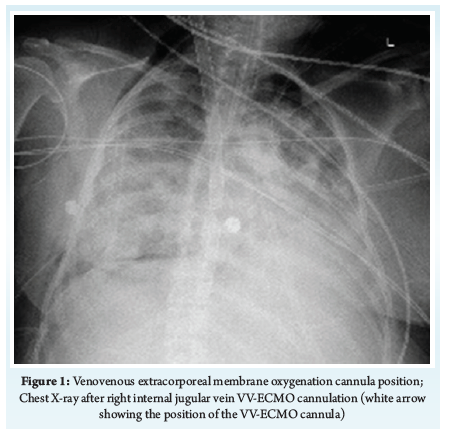
The patient had continued deterioration of her respiratory status with worsening partial pressure of oxygen and fraction of inspired oxygen ratio (PaO2/FiO2) despite maximal conventional therapy including paralysis, inverse ratio pressure control ventilation, and a FiO2 of one. The worsening hypoxia evident in the SpO2, PaO2, and PaCO2 on the multiple arterial blood gases (ABG) showed her quick deterioration. The patient had an acute decompensation with an ABG showing 7.17/8.6/93/30/0. Cardiothoracic surgery was consulted for possible VV-ECMO, and a subsequent ABG with patient on 100% FiO2 showed 7.41/52.3/69/33.2/7.4. The decision was made to cannulate the patient as there was no reserve from either a patient or ventilator perspective. Therefore, due to respiratory failure with persistent poor oxygenation despite being maximally supported on the ventilator, she was placed on VV-ECMO via a right internal jugular 32 French Crescent cannula (Fig. 1) on day seven. With the limit of ventilator manipulations met, the potential benefits of VV-ECMO to the mother and baby outweighed the risks of initiation.
Therapeutic anticoagulation was initiated with heparin. She was also found to be bacteremic with Methicillin-susceptible Staphylococcus aureus and was started on cefazolin. Two days after VV-ECMO initiation, non-reassuring fetal heart tones necessitated emergent non-sterile bedside low transverse C-section at 27.2 weeks’ gestational age in the intensive care unit. Appearance, pulse, grimace, activity and respiration (APGAR) scores of the newborn were two, five and seven at one, five and ten minutes, respectively. The patient’s respiratory status and hemodynamics subsequently improved following the delivery. The patient made a significant improvement in oxygenation and ventilation immediately after C-section, and then subsequently a more gradual improvement as seen with other COVID-19 patients up until the time of decannulation.
On day 23, 13 days post C-section, the patient was decannulated from VV-ECMO. Subsequently, the patient displayed tremendous improvement in endurance and was ready to be discharged to the local Ronald McDonald House to remain her to her baby boy while he was in the neonatal intensive care unit.
Discussion:
The obvious benefit of proceeding with this emergent bedside C-section was to save the fetus. However, this had to be weighed against the risks of hemorrhage in this high-risk patient since she had two previous C-sections and was on a therapeutic heparin drip while on VV-ECMO. To note, the C-section was not considered before the commencement of VV-ECMO despite anticipated use of heparin because the plan was to allow the fetus to have as much time to mature as possible. However, the team knew that the possibility of requiring the C-section was not low, and hence dexamethasone was administered for fetal lung maturity. Concerning fetal outcome, the fetus did well post-utero and is alive. The intervention was obviously beneficial to the fetus as it was in distress due to fetal bradycardia while in utero, which prompted the emergent C-section.
In a 2011 case report of a C-section done on a woman placed on VV-ECMO due to respiratory distress syndrome from the A/H1N1 flu, the patient was successfully weaned from ECMO one week after delivery and was discharged home 8 weeks from admission without oxygen support and there was good fetal outcome [7].
An additional risk to consider was the possibility of infection due to having the C-section done in a non-sterile manner, especially in a patient who was bacteremic. This was mitigated by using additional prophylactic vancomycin peri-operatively.
The patient’s respiratory status improved significantly after the fetus was delivered, likely due to improvements in respiratory mechanics post-partum. Following a C-section, uterine contractions may increase venous return and cardiac output. However, compared to vaginal delivery, little is known about hemodynamics after C-section. Additionally, while pregnancy may predispose women to being infected with COVID-19 and developing severe COVID-19 clinical events due to altered immune and respiratory functioning, increasing data has shown that pregnant women without underlying comorbidities are not disproportionally affected by COVID-19 complications [11, 12]. Thus, more data is necessary to gain a better understanding of the effect of COVID-19 on pregnancy.
The successful outcome of this patient and her baby required the timely coordination of a multidisciplinary team including the intensivists, cardiothoracic surgeons, obstetricians, nurses, and operating room technicians. Key factors to this favorable outcome include the timely initiation of VV-ECMO, meticulous continuous fetal monitoring which enabled prompt recognition of fetal distress and activation of the obstetric team for C-section, as well as effective communication between the various teams which minimized unnecessary delays.
Strengths of this case report include that we have provided an organized, and detailed timeline describing this patient’s need to be placed on VV-ECMO and ultimately have an emergent Cesarean-section. Due to the extremely limited data on Cesarean-sections for patients on VV-ECMO, this case report provides additional information and outcome data for this rare event.
A limitation of this report is our inability to establish a definite cause-effect relationship between the intervention and outcome of the patient. Additionally, the positive outcome of this patient was dependent on multiple factors and may not be easily replicated in a different clinical setting.
Conclusion:
Emergent C-section on a pregnant woman with respiratory failure on VV-ECMO can be life-saving for the fetus and the mother. However, the inherent risks associated with it requires close monitoring of the patient and the fetus in order to determine when this is truly necessary and beneficial.
Clinical Relevance:
ECMO is associated with low risks of maternal and fetal complications in well-selected pregnant and postpartum patients. The benefits and drawbacks of Caesarean-section on VVECMO should be evaluated from a multidisciplinary view. Despite that the immediate hemodynamic changes after C-section delivery are still not as well understood, the limited publications available about Caesarean-sections on VVECMO state that delivery helped expedite the hemodynamic statuses of the mothers off VVECMO as seen in our patient.
References
[1] Supady, Alexander et al. “Respiratory indications for ECMO: focus on COVID-19.” Intensive care medicine, 1–12. 9 Aug. 2022, doi:10.1007/s00134-022-06815-w.
[2] Sharma, N. S., Wille, K. M., Bellot, S. C., & Diaz-Guzman, E. (2015). Modern use of extracorporeal life support in pregnancy and postpartum. ASAIO journal (American Society for Artificial Internal Organs : 1992), 61(1), 110–114.
[3] Banfi, C., Pozzi, M., Siegenthaler, N., Brunner, M. E., Tassaux, D., Obadia, J. F., Bendjelid, K., & Giraud, R. (2016). Veno-venous extracorporeal membrane oxygenation: cannulation techniques. Journal of thoracic disease, 8(12), 3762–3773.
[4] Extracorporeal Life Support Organization ELSO Guidelines. [Jul;2019 ];https://www.elso.org/Resources/Guidelines.aspx 2019.
[5] Naoum, Emily et al. “Extracorporeal Life Support in Pregnancy: A Systematic Review.” American Heart Journal, 9(13). July 2020, https://doi.org/https://doi.org/10.1161/JAHA.119.016072
[6] Aissi James, S., Guervilly, C., Lesouhaitier, M. et al. (2022). “Delivery decision in pregnant women rescued by ECMO for severe ARDS: a retrospective multicenter cohort study.” Crit Care26, 312. https://doi.org/10.1186/s13054-022-04189-5
[7] “CDC Covid Data Tracker.” Centers for Disease Control and Prevention, Centers for Disease Control and Prevention, 22 July 2022, https://covid.cdc.gov/covid-data-tracker/?CDC_.
[8] Panarello, G., D’Ancona, G., Capitanio, G., Occhipinti, G., Attardo, G., Bertani, A., & Arcadipane, A. (2011). Cesarean section during ECMO support. Minerva anestesiologica, 77(6), 654–657.
[9] Stiff, A., Harrison, R., & Palatnik, A. (2019). Case report of massive hemoptysis in pregnancy requiring veno-venous extracorporeal membrane oxygenation. The journal of obstetrics and gynaecology research, 45(12), 2452–2455.
[10] Quintero, Alejandro et al. “Extra-corporeal membrane oxygenation and emergency C-section for a pregnant COVID-19 positive patient.” Perfusion, 2676591211049769. 7 Oct. 2021, doi:10.1177/02676591211049769
[11] Santa, S., Doku, D. A., Olwal, C. O., Brown, C. A., Tagoe, E. A., & Quaye, O. (2022). Paradox of COVID-19 in pregnancy: are pregnant women more protected against or at elevated risk of severe COVID-19?. Future microbiology, 17, 03–812. https://doi.org/10.2217/fmb-2021-0233
[12] Wang, C. L., Liu, Y. Y., Wu, C. H., Wang, C. Y., Wang, C. H., & Long, C. Y. (2021). Impact of COVID-19 on Pregnancy. International journal of medical sciences, 18(3), 763–767. https://doi.org/10.7150/ijms.49923
| How to Cite this Article: Myles A, Ang SS. Emergent Bedside Cesarean Section for COVID-19 Patient on Veno-venousExtracorporeal Membrane Oxygenation: A Case Report. Journal of Anaesthesia and Critical Care Case Reports. January-April 2024; 10(1): 05-07. https://doi.org/10.13107/jaccr.2024.v10.i01.229 |
(Article Full Text HTML) (Download PDF)