Vol 4 | Issue 1 | Jan-Apr 2018 | page: 21-30 | Sandeep Diwan, Chetan Pradhan, Atul Patil, Chetan Puram, Parag Sancheti
Authors: Sandeep Diwan [1], Chetan Pradhan [2], Atul Patil [2], Chetan Puram [2], Parag Sancheti [3]
[1] Department of Anesthesia, Sancheti Hospital for Specialised Surgery, Pune, Maharashtra, India,
[2] Department of Orthopaedics, Sancheti Hospital for Specialised Surgeries, Pune,Maharashtra, India.
[3] Proffesor and Chairman and Sancheti Hospital for Specialised Surgeries, Pune,Maharashtra.
Address of Correspondence
Dr. Sandeep Diwan,
Department of Anesthesia,
Sancheti Hospital for SpecialisedSurgery, Pune, Maharashtra, India.
Email: sdiwan14@gmail.com
Abstract
The geriatric population with its multiple comorbid conditions are at risk of developing anesthesia-related complications. Data are inconclusive as to whether a general anesthesia , epidural or spinal (regional) anesthesia improves outcomes after hip fracture surgery. The author ( S M D ) subjected all ASA grade 3 and 4 intertrochanteric fractures to lumbosacral plexus block. Intraoperative haemodynamic stability was a key feature in all the patients which reflected in a stable postoperative scenario. The positive outcome, early patient – relative interaction and day 2 assisted mobility of the patient lead to an increase in demand for lumbosacral plexus block in high risk geriartrics with intertrochanteric fractures.
Keywords: Fractures of intertrochanteric, local anesthesia, lumbar plexus block, nerve block, post-operative pain relief, sacral plexus block.
Introduction
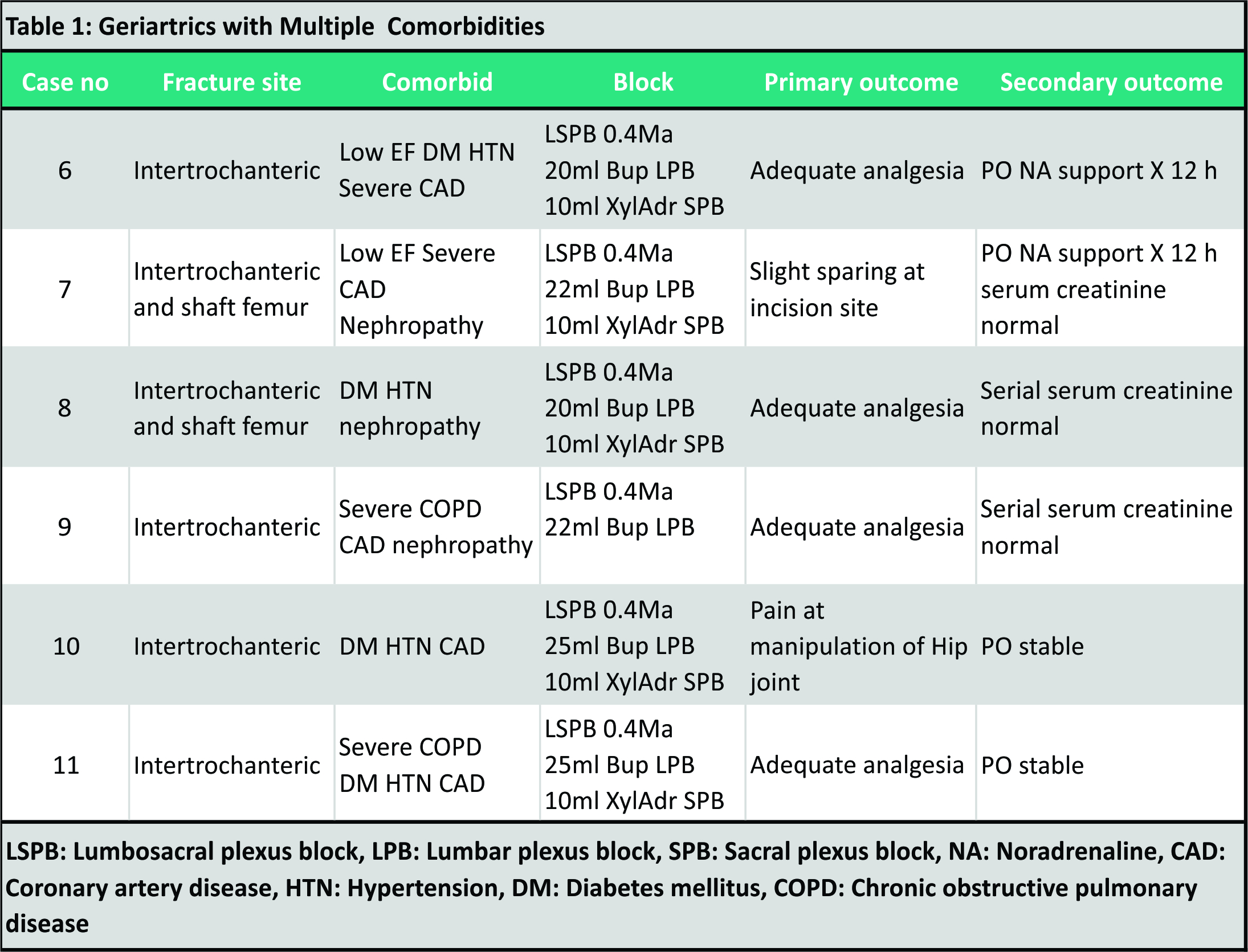
In this case series stretching from January 5, 2015 to January 31, 2017, the author presents 50 high-risk patients with multiple comorbidities listed for repair of fractured intertrochanteric with open reduction and internal fixation. All the surgical procedures were performed under a combined lumbosacral plexus block (SPB). None of these patients received a general anesthetic. The first 5 complex cases are discussed in this article. The other 6/50 cases are listed in Table 1.
All the 50 patients had uneventful recovery and were discharged to the ward/room following their initial stay in the critical care unit. The techniques of lumbosacral plexus block (LSPB) in fracture hip surgeries will be discussed along with existing evidence, complications, controversies, and suggestions evolving around the LSPB.
Case Reports
Case 1
A 78-year-old female with severe hypothyroidism was admitted with a right fracture intertrochanteric. On admission her thyroid-stimulating hormone (TSH) was >100 ulU/ml, she was placed on thyroxine,and 5 days later her TSH revealed 84.55ulU/ml (0.27–4.2 ulU/ml). Thyroid function tests revealed free thyroxine 0.39ng/dl,free triiodothyronine8.78pg/mlandan intact parathyroid hormone level 252.7pg/ml (9–65pg/ml).Serum creatinine 1.0mg/dl and serumalkalinephosphatase 273IU/L were the latest reports before going in for the surgical procedure. The electrocardiogram (ECG) revealed a left anterior hemiblock, and an echocardiograph demonstrated a concentric left ventricular hypertrophy and an ejection fraction of 32% with inferoapical hypokinesia. Her chest X-ray revealed a calcified aortic wall. A lumbar X-ray revealed scoliotic deformity (Figure. 1). Considering her long-standing hypothyroidism and low ejection fraction with regional wall motion abnormalities an unstable hemodynamics was anticipated under a spinal or an epidural. In spite of the severe scoliosis, an attempted lumbosacral plexus was successful. The anatomical landmarks did not correlate to internal endpoints (Figure 1 ). The needle insertion would have been too lateral according to the anatomical landmarks. Total volume for Lumbar plexus block – 14ml 0.5% Bupivacaine Total volume for Sacral plexus block – 10ml 0.5% Bupivacaine
The anatomical landmark for the proposed LPB did not correlate to the point of needle insertion (Fig. 1).

Case 2
A 80-year-old male with prior history of renal dysfunction was admitted with a left intertrochanteric fracture. Blood investigations revealed hemoglobin (Hb)- 8.5g/dl, BUL- 80mg/dl,and serum creatinine 3.0mg/dl. Echocardiograph mentioned left ventricular ejection fraction- 28%, left ventricular diastolic dysfunction (LVDD) was GradeIII, left ventricular hypertrophy and mild regurgitation across mitral and tricuspid valves. Ultrasound of the abdomen diagnosed bilateral hyperechoic renal parenchyma and altered corticomedullary differentiation. This was suggestive of the bilateral renal disorder. A medical consultation advised against theuse of nonsteroidal anti-inflammatory drugs, aminoglycosides and avoids hypotension and hypoxia. A neurostimulation guided LSPB was administered. Total volume for Lumbar plexus block – 15ml 0.5% Bupivacaine Total volume for Sacral plexus block – 10ml 0.5% Bupivacaine. The surgical procedure was uneventful. Postoperative analgesia lasted for 14 hours without the need for opiates. The haemodynamics was stable perioperatively.
Case 3
A 80-year-old female with severe bronchial asthma not responding to bronchodilators,steroids and nebulization was posted for open reduction and fixation of the intertrochanteric fracture. ECG revealed a left bundle branch block (Fig. 2). Echocardiograph suggested sclerotic aortic valve with a pressure gradient of 50mmHg, associated mitral and tricuspid regurgitations , a Grade III LVDD and an EF of 35%. Her arterial pressures on admission were 210/100,and subsequent readings were 160/94. Counseling was performed,and she was posted for asurgical procedure under a LSPB. A neurostimulation guided LSPB was administered. Total volume for Lumbar plexus block – 18ml 0.5% Bupivacaine Total volume for Sacral plexus block – 8ml 0.5% Bupivacaine Atrial fibrillation persisted in the perioperative period, though the haemodynamics was well maintained.
Case 4
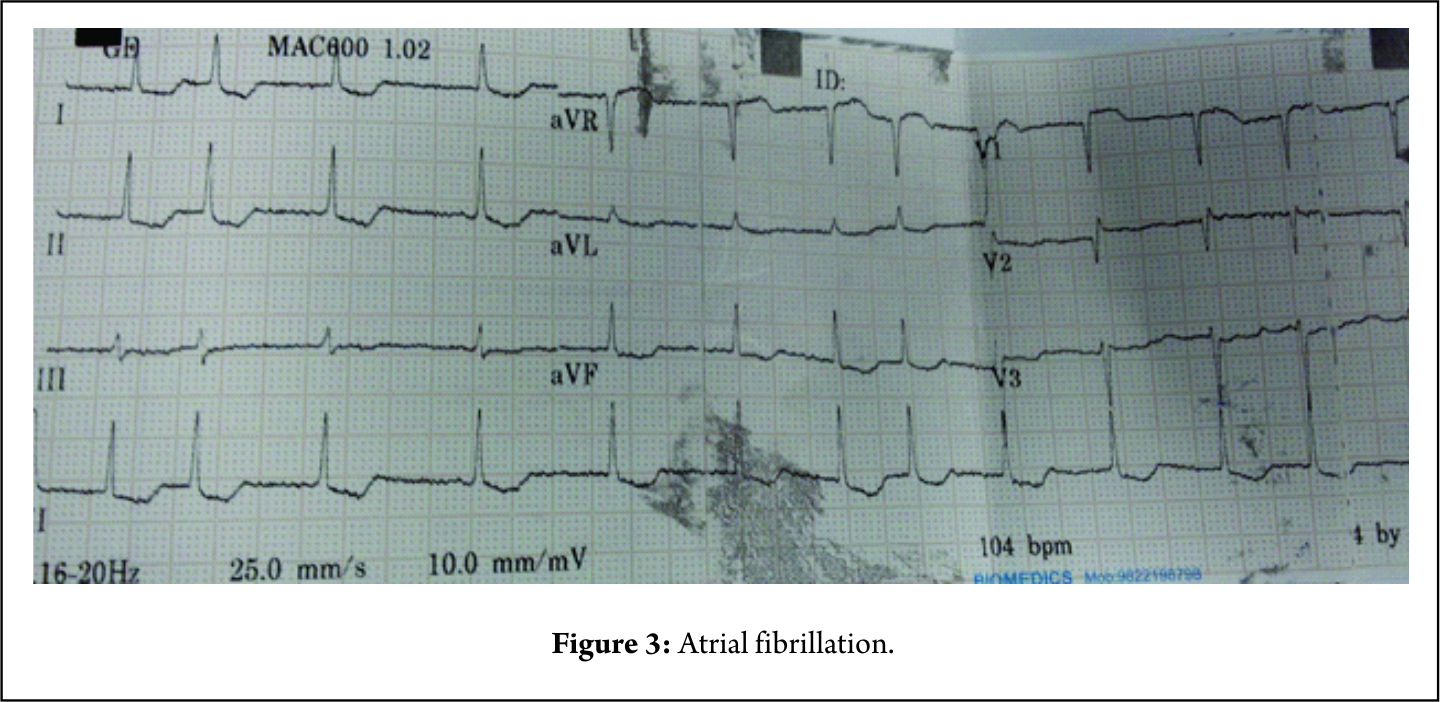
A 92-year-old female is known hypertensive and with a history of myocardial infarction 35 years back suffered from intertrochanteric fracture. At the time of admission, her ambulatory blood pressure (ABP) was 130/80,heart rate 82/min, and oxygen saturation was 92% on air. Her examination of cardiovascular system, respiratory system, and central nervous system was normal. A computed tomography (CT) scan brain was normal. At admission, she was on lanoxin 0.25mg per day. An ECG revealed chronic atrial fibrillation pattern and a 2D echocardiography revealed an EF of 45%, a Grade III LVDD, a moderate tricuspid regurgitation and RVSP of 40mm Hg (Fig. 3).
She was transfused two pints of RBCs on which her Hb improved to 8.8mg/dl and packed cell volume (PCV) to 24%. Her blood urea was 28mg/dl, serum creatinine 0.8mg/dl. She was hyponatremic with a serum Na of 120mEq/L on admission and hypochloremic with serum Cl of 87mEq/L. This was corrected over 3 days of admission with 1000ml of NaCl every day. Her pro-brain natriuretic peptide was on the higher side (583pg/ml – normal 125pg/ml), and anINR was within normal limits (1.15). The right radial artery was cannulated for continuous arterial pressure monitoring.The patient was positioned in the right lateral position. A neurostimulation guided LSPB was performed. A neurostimulation guided LSPB was administered. Total volume for Lumbar plexus block – 12ml 0.5% Bupivacaine Total volume for Sacral plexus block – 8ml 0.5% Bupivacaine She was shifted from post-anesthesia care unit after 2 h of close observation to surgical ICU for 48 h observation. Post-operative she had an episode of supraventricular tachycardia which was controlled with a bolus of amiodarone followed by 2 days of amiodarone ( fig 4 ) infusion. She was discharged from the surgical intensive care unit (SICU) on the 4thpost-operative day with a sinus rhythm and off medications (Fig. 4).
Case 5
A 85-year-old female suffering from long-standing hypertension and ischemic heart disease. She had a recent episode of the acute coronary syndrome which coincided with a fall following which she suffered a from left fracture of left intertrochanter. At the time of admission, she was on diuretics, low-molecular-weight heparin (LMWH), antihypertensive, and antianginal. Her Hb was 6 and was transfused 2 pints of PCV. HbA1C was 6, serum creatinine 1.1,serum Na 130,serum K 3.7, and serum bilirubin 0.4. Her pro-BNP was strongly positive at 7666,and Trop T was weakly positive. ECG revealed inferior ST-T changes and echocardiograph suggested inferior akinetic wall, and an EF of 26%, a moderate to severe mitral regurgitation and a moderate pulmonary hypertension. Chest X-ray revealed cardiomegaly and ultrasound pelvis suggested a single kidney. After a A radial artery cannulation was performed for invasive monitoring of A B P. A left LSPB was administered with 0.5% bupivacaine 20ml and 1.5% xylocaine ( 12ml for LPB and 8 ml for SPB ) under neurostimulation guidance with endpoints at 0.4Ma.The LSPB was adequate for asurgical procedure. A cardiologist was standby throughout the surgical procedure. Post-operative she was shifted to SICU and was under observation for 48 hours. All the patients were administered subcutaneous 0.2mg to 0.4mg enoxaparin8 h after the surgical procedure.
Technique of LSPB
Positioning of the patient
Prior to positioning titrated doses of intravenous midazolam 1mg and fentanyl 25–50mcg are administered to provide conscious sedation. Alternatively a femoral nerve block with 1% xylocaine 10ml is administered in supine position. The patients are positioned in lateral with the operating side up. The intramedullary nail for all fractures intertrochanters are performed in the lateral position by our surgeons. Note the patient is stabilized with a posterior and anterior support. The non-fracture hip is flexed, the fractured limb is kept straight and supported by a pillow underneath. Prior to positioning titrated doses of intravenous midazolam 1mg and fentanyl 25–50mcg are administered to provide conscious sedation. A neurostimulation modality is chosen for all LSPB. The plexus blocks are performed using a 100mm insulated needle <H2>The lumbosacral line (Fig. 5)
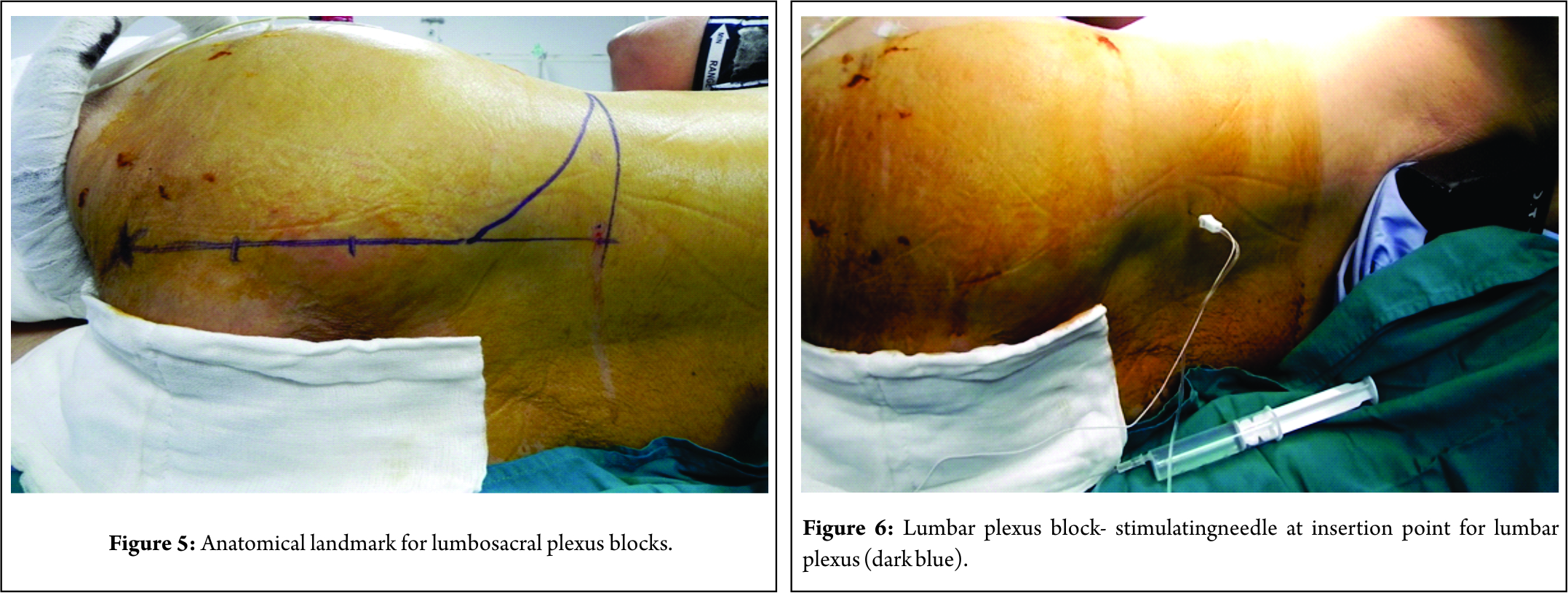
The lumbosacral line (Fig. 5)
Lumbar plexus anatomical landmark
An intercristal line is drawn. A line is drawn cephalad from the posterior superior iliac spine (PSIS). These lines intersect at one point which is the point of needle insertion for the LPB.
Sacral plexus anatomical landmark
A line is drawn from the PSIS to the ischial tuberosity (IsT). This is divided into three parts. A point is chosen proximal one-third on this line and is the point of needle insertion for the SPB. Not mentioned is the literature is the peculiar “lumbosacral line.” As depicted in the figure the points of needle insertion for LPB (dark blue arrow) and SPB(dark yellow arrow) lie on the same line.
PSIS: Posterior superior iliac spine.
Blue arrow – Needle insertion for Lumbar Plexus Block.
Dark Yellow – Needle insertion for Sacral Plexus Block.
Techniques
LPB (Fig. 6)
A 100mm stimulating needle is inserted at the mentioned point(intersection of anintercristal line and the line drawn through the PSIS).The needle makes its way through muscles of the back until it encounters the transverse process (this osseous contact is of immense importance). The needle tip is inserted not more than 1.5 to 2cm beyond the transverse process. The evoked muscle response during a LPB is quadriceps contraction at 0.4mA. The volume of local anesthetic injected is 20–25ml of 0.5% bupivacaine.
Contrast study of LPB(Fig. 7)
A contrast study performed during a LSPB whenever the serum creatinine levels were below 0.5mg%. The contrast spread reveals the spread across the lumbar plexus and sharply delineates the compartment where the lumbar plexus is located. The quadriceps response was obtained at 0.4 Ma in this contrast study. The contrast spreads cephalad to the level of L2 in the retroperitoneal area of the origin of psoas and the commencement of the lumbar plexus elements. This is close to the neuraxis. Distally there is an intrapelvic spread upto the lower border of L5. The spread confirms the blockade of the femoral and the lateral femoral cutaneous nerve (LFCN), but, the blockade of the obturator is doubtful since the location of this nerve is more medial. The proposed point of needle insertion (Winnies) lies just lateral to the lateral margin of the contrast. This suggests a slight medial deviation of the needle tip is required.

SPB (Fig. 8)
The anatomical landmark of needle insertion (line joining the PSIS and the IsT, is divided into three parts, the needle insertion is the point of proximal one-third and the distal two-thirds on this line). The stimulating needle is inserted perpendicular to the gluteal muscles, and if hits the sacral plate the needle tip should not be more than 1.5–2cm beyond the sacral plate. The evoked muscle responses are either the plantar flexion or the dorsiflexion of the foot at 0.4mA. The volume of local anesthetic injected is 0.5% bupivacaine.
Contrast study of the SPB (Fig. 9)
A contrast study performed during a SPB identifies the intra- and extra-pelvic spread of the local anesthetic. The intrapelvic spread blocks the gluteal and pudendal nerves, and the distal sciatic spread blocks the posterior cutaneous nerve of thigh and the main sciatic nerve.
The assessment of sensory and motor functions was made by assessing the incisional part with a cold sponge, gentle pinching of the concerned area and gently moving the fractured limb. Sparing of the incisional area was observed in more than 50% and is the area of major concern. The patients were able to move the contralateralleg and complained of it being cold. All the patients were hemodynamically stable with a slight fall in the arterial blood pressure ABP (8–10mmHg). In three patients the drop in APB was significant (>30mmHg). This probably suggested an epidural spread and was evaluated in the post-operative period. The contralateral limb extension was minimally restricted and was confirmative of possible epidural spread.
Discussion
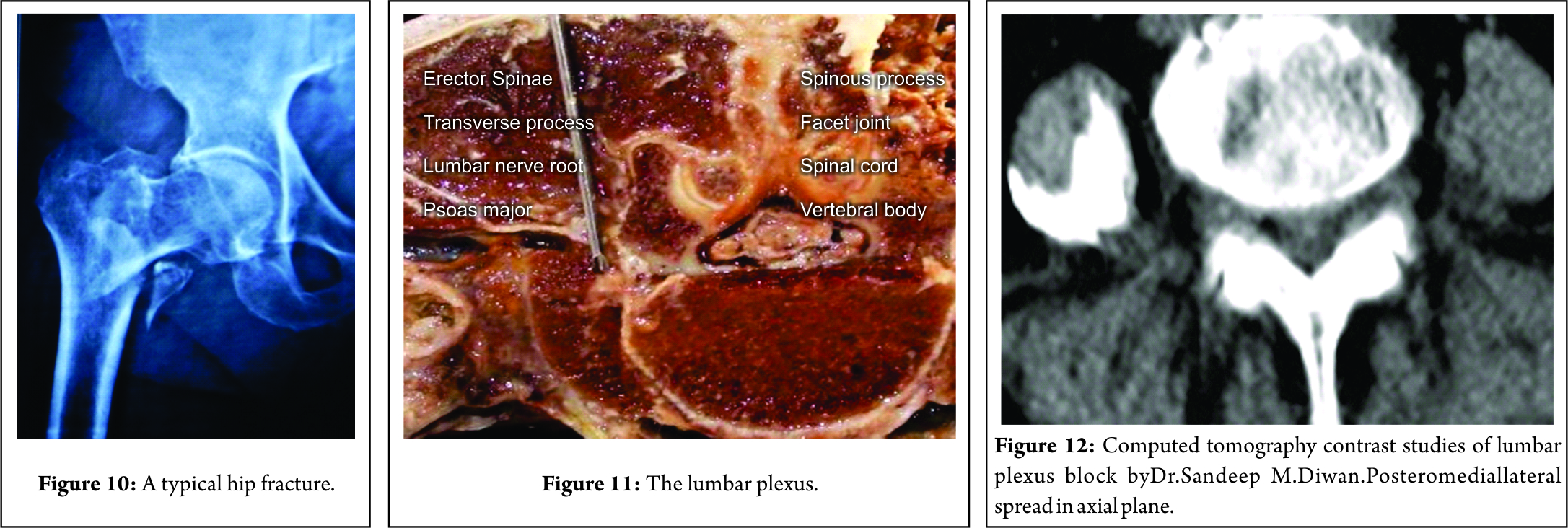
Hip fracture prevalence is rising with the continued aging of the population [1]. Studies [2,3] have demonstrated the increased risk of mortality after hip fracture especially during the 1styear, and excess mortality risk may persist for several years after fracture. Age [4,5] itself is a major determinant of outcome in patients with fractured neck of femur, but how it influences the primary decision to proceed with surgery cannot be measured. Oliveret al.[6]report a 113 years woman admitted with fracture neck femur successfully received a morphine based anesthesia, in a superior physiological condition. The authors conclude that age alone should not be a bar to surgery. The timing of surgical intervention is of utmost importance considering the risk of mortality involved in delayed interventions. A meta-analysis [7] published in 2010 investigating the effect of surgical delay on mortality at different follow-up times, found significantly higher all-cause mortality for patients treated surgically more than 24, 48, and 72 h from admission. Lee and Elfar [8] examined the current literature to define the relationship between the timing of hip fracture surgery with mortality, length of hospital stay, and post-operative complications. With several supporting studies they conclude that early surgery within 48 h of admission decreases the length of hospital stay, incidence of bed sores and provides early return to independent living. Historically, general anesthesia[10] has been the gold standard for surgeons and patients for when major hip surgery (Fig. 10) is being done. General anesthesia is an alternative but the anesthetic agents can depress the myocardium, produce profound vasodilatation and can be associated with a stormy perioperative course. The use of a mainly opioid-based anesthetic does not guarantee hemodynamic stability and may delay emergence. The use of epidural or spinal anesthesia[10] during major hip surgery is associated with a reduced risk of perioperative complications such as deep venous thrombosis, less deterioration of cerebral and pulmonary functions in patients who are at high risk for complications. The Neuraxial blocks ( NAB – spinal and epidural) are commonly used for surgical repair of hip fracture. A recent meta-analysis [11] of randomized controlled trials comparing general anesthesia with regional anesthesia for hip fracture surgery concluded that there are marginal benefits of using the latter in terms of early mortality and risk of deep vein thrombosis. However,the most important observations were there was trend toward a lower incidence of myocardial infarction, confusion, and post-operative hypoxemia in patients who receive regional anesthesia. NAB is supposed to reduce mortality. The overall mortality rates of GA patients, NAB patients, and continuous peripheral nerve block patients were 69.6%, 36%, and 33.7%, respectively (1 month and 1 year mortality rates).The effects of LSPB on mortality in hip fractures are not yet studied. Spinal anesthesia is purposefully avoided by this author in high-risk geriatrics for hip fractures. It produces profound vasodilatation below the level of the block, resulting in hypotension, which may be exacerbated and have negative implications in patients with multiple comorbidities. Even a lowest volume 1.2ml 0.5% bupivacaine administered slowly produced significant hypotension (mean arterial pressure<60mmHg) requiring the need for vasopressors in the perioperative period extending to the post-operative period in the SICU. This author prefers a segmental lumbar epidural as opposed to spinal anesthesia for high-risk patients (ASA 111-1V ) with hip fractures. A close hemodynamic monitoring, careful titration of local anesthetic dose and pharmacological support, an epidural technique has have been used successfully in patients with fracture hip with multiple comorbid. The maximum volume of local anesthetic used was 14ml 0.5% bupivacaine in 98-year-old male and the minimum volume used was 6ml 0.5% bupivacaine in 97-year-old female. In both the patients the epidural was instituted at L2-3 interspinous level. The surgical procedure a proximal femoral nail lasted for a total of 35min and 38 minutes, respectively. Except for a fall of ABP of 10–15mm Hg at the 20–22nd min, hemodynamically all the patients in epidural group were stable.
There are certain geriatric patients who suffer from hip fractures and are a strong contraindications for neuraxial techniques particularly the “Epidurals.” According to this author, three categories are defined where an epidural is contraindicated, and patients are best subjected for a LSPB.
A) Patients on low molecular weight heparins who cannot be weaned off or require a bridging therapy. The patients on LMWHs are the ones with risk of epidural hematomas. The last dose of LMWH received is 10h before the single shot LSPB.
B) Patients who have regional wall motion abnormalities and very low ejection fraction of < 25 are the ones who may not cannot tolerate epidural related sympathectomy.
C) Patients who have operated spine with hardware in situ with or without lower limb neurological symptoms and signs, are the ones in whom it is difficult to gain access to the spinal or epidural space, the spine is best left untouched.
The question remains whether a large volume and technically challenging LSPB is more effective and safe technique than the epidural? A comparative study between the above two techniques is not possible in a high risk group of patients. In this article, the author reports the successful use of a combined lumbar plexus and SPBs(LSPB) for operative repair of hip fracture in an elderly patients with multiple comorbids. Significantly all the patients remained awake throughout the surgical procedure. Apart from the cases mentioned above, patients with acute coronary syndrome, severe pulmonary hypertension (pulmonary artery pressure=70mmHg), severe chronic obstructive pulmonary disease (with h/o recent ventilator therapy), left ventricular failure (raised BNP ≥ 5000) received a lumbosacral block. The author chose to use a combined LSPB because it produces complete anesthesia of the ipsilateral lower limb effective for surgical repair of hip fracture, provides stable hemodynamics in the perioperative period and excellent post-operative pain relief along with non-opioid analgesics. There are numerous case reports [14-16] and series [13,17] especially for high-risk geriatric patients who suffered from hip fractures and underwent a surgical procedure under lumbar and sciatic/SPB. All the concerned literature mentions that the minimal hemodynamic disturbance and cardiovascular stability are the advantages of LSPB when compared with GA and NAB. deVismeet al. [13] studied prospectively in a randomized designed to determine the hemodynamic effects and quality of combined LSPB compared with plain bupivacaine spinal anesthesia in the elderly for repair of proximal femoral fractures. They conclude that hypotension was found to be longer lasting after spinal anesthesia and of a larger magnitude in patients over 85 years of age. This is advantageous in patients with severe aortic stenosis since they tolerate hypovolemia poorly. There are increasing number geriatric patients with hip fractures, asymptomatic and are diagnosed with mild-severe form of aortic stenosis. in the pre-operative evaluation. LSPB , considering the haemodynamic stability could be valuable in this scenario. The unilateral block leads to a lower incidence of urinary retention and less changes in systemic vascular resistance compared to central NAB[19,20].
LPB HIP innervation
The sensory innervation of the hip is derived from branches of both the lumbar and sacral plexus. The anteromedial innervation of the hip joint capsule is by the articular branches of the obturator nerve and the sensory articular branches from the femoral nerve [21]. The posterior and the posteromedial part by the articular branches from the sciatic nerve and the nerves to the quadratus femoris muscle [21]. The articular branches of the superior gluteal nerve innervate the posterolateral section of the hip joint capsule [21]. Lumbar plexus blockade has been shown to be reliable in blocking major branches of the lumbar plexus (femoral, lateral femoral cutaneous, and the obturator nerves) and the SPB(sciatic, posterior cutaneous nerve of thigh, gluteal, and pudendal nerves) [22,23]. A LSPB is thus ideal for the hip fractures if a spinal and even an epidural are contraindicated. In case 1, 24, and 46 with marked scoliosis (representative Fig. 1), the anatomical landmark of needle insertion (needlepoint insertion is the point of intersection of anintercristal line and the line passing through the PSIS) did not correlate to the needle insertion and was too lateral. It was decided to place the needle a bit medially, hit the transverse process and negotiate the tip into the posterior psoas major to identify the lumbar plexus. In the other 47cases, there were no anatomic abnormalities in the spine. In a normal back, the external anatomical landmarks exactly correlate with the internal target points ( lumbar plexus ). This was appreciated in all the 47 cases. The lumbar nerves exit the intervertebral and lie in the posterior one-third of the psoas major muscle to eventually form the lumbar plexus(Fig. 11). The psoas major muscle is situated in front of the transverse process (Fig. 11). Thus, a stimulating needle will always contact the transverse process and is then negotiated in either below or above the transverse process to enter into the psoas major (Fig. 11). The distance of lumbar plexus from the transverse process is fixed and is at 1.5–2cm (Fig. 11).
Cadaveric dissection by Dr.SandeepDiwanMiraj.
The neurostimulation endpoint of LPB at 0.4mA is quadriceps contractions. After stabilizing the needle tip, 20ml of 0.5% bupivacaine is injected.
Radiological studies
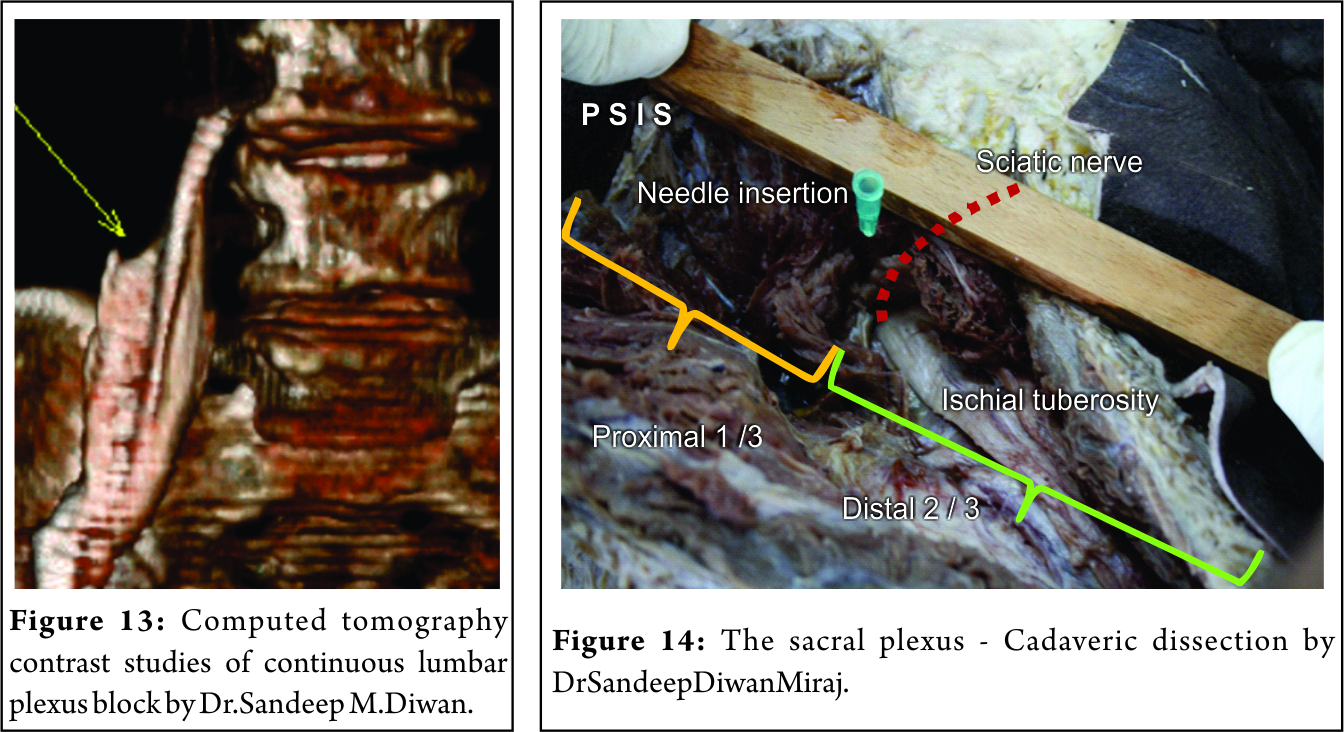
Capdevila et al.[24]have used CT imaging to investigate the performance of psoas compartment block (PCB) in adults. The depth of the lumbar plexus from the skin was 61–101 mm in men and 57–93 mm in women, providing a guide to the depth of needle insertion. This author has earlier performed several contrast studies of the LPB (Fig. 12 and 13). The medial spread to the neuraxis was found in only 6 patients. All the spread were linear and sharp in the middle of the psoas muscle. In some CT contrast, the spread was medial in the coronal plane (Fig. 13) and posterior aspect in the axial plane (Fig. 12).This explains the blockade of the femoral, LFCN and the obturator nerve as the contrast spreads posteromediolateral in the psoas muscle.
Extent of the blockade in LPB
Mannion et al.[27]compared the approaches of Winnie and Capdevila for PCB in terms of contralateral spread, lumbar plexus blockade, and post-operative analgesic efficacy. Bilateral anesthesia occurred in 10 patients in Capdivella approach and blockade of femoral, lateral femoral cutaneous, and obturator nerves was 90%, 93%, and 80%, respectively. In Winnies group 12 patients had bilateral block and 93%, 97%, and 90% had femoral, lateral femoral cutaneous, and obturator nerves, respectively. The psoas muscle gets cleaved after administration of solution within the fascial plane [27].This facilitates the distribution of solution to the lumbar nerve roots. This mechanism of spread [27] to the nerve roots ensures that obturator nerve block occurs in 85–90%. The obturator nerve is outside the psoas fascial plane in a separate fascial sheath [27].
Sacralplexus
The sacral plexus exits at the greater sciatic notch (Fig. 14). A line joining the PSIS and the IsT is divided into three parts (Fig. 14). The needle is inserted at proximal 1/3rdand distal 2/3rdon this line (Fig. 14). The needle at times hit the sacral plate and negotiated toward the sacral plexus directing caudad. The proximal one-third point on the line joining the PSIS and the IsT correlated with its internal target the sacral plexus. A small deviation of 10° was needed either medially or laterally in the lumbar plexus block and 10–20° caudad or superior in the SPB.
Sparing
This authors previous experience with LSPB for hip surgeries suggested sparing of the lateral incisional area (complexly innervated by the LFCN of thigh, the subcostal and the ilioinguinal nerves). This was taken care of with a separate block of the LFCN at 2cm medial and inferior to the anterior superior iliac spine with 10ml 0.25% bupivacaine and or local anesthetic infiltration at the surgical site with 5ml 1% xylocaine. Thus a total of 35–40ml of local anesthetic compound solution of 0.5% bupivacaine and 1.5% xylocaine with or without adrenaline was utilized.
Complications
Two important complications are to be taken into consideration during every LPB. Epidural spread [34] because injections are in close vicinity of neuraxial space and local anesthesia systemic toxicity (LAST) since injections are made in the highly vascularized area[28,29]. Aspirating the needle or catheter before each injection and administering local anesthetic in 3–5 ml aliquots is advised in the ASRA Practice Advisory [31] on LAST and may be useful in limiting intravascular injection. However, arrhythmias have been reported after PCB despite a negative aspiration test and the use of divided doses [29].
Reasons for neuraxial spread
The PCB is a paravertebral blockade of the lumbar region [36]. The paravertebral space lies in continuity with the epidural space [36]. Dural sleeves might extend as far as the paravertebral area thus communicating freely with the neuraxial space [36]. A medially directed needle according to this author has high probability of epidural spread, this is also confirmed by others [24].The injection of local anesthetic with high injection pressures (>20 psi) may result in the unintentional bilateral blockade and an increased risk of neuraxial blockade[38]. A larger local anesthetic volumes increase the likelihood of epidural spread [39]. Ultrasound localization has enhanced understanding of needle–nerve relationships [37]. It allows clear delineation of paravertebral anatomy as well as real-time views of block needle advancement and local anesthetic distribution during injection [37]. Karmakar et al.[37] performed LPBs on undergoing emergency lower limb surgery. In three of five patients, the lumbar plexus nerve roots were identifiable by ultrasound in the posterior aspect of the psoas muscle. Thus improved nerve localization may allow for targeted administration of lower doses of local anesthetic medication, lessening the risk of LAST and injecting with low pressures will probably decrease the incidence of the epidural spread. In this authors practice the LPB receives a maximum of 22–25 ml in Indian patients. The least volume used by this author was 12 and 14ml for LPB and 6 and 8ml for a SPB in female patients weighing 28 and 30kg, respectively. In this author series as the blocks are performed in the lateral position with the operating side up there is increased chances of the drug spreading into the epidural space along a vertical and concentration gradient. The volume of drug used is 22–25ml injected ultra slow, as against the reported 40ml in literature [40].
Haemodynamic Stability
In the elderly patients, with pre-existing hypovolemia or general debilitation, severe cardiovascular collapse may ensue after a N A B. All the patients in this study of high-risk geriatric hips anesthetized with a LSPB demonstrated a remarkable stable hemodynamics with a maximum drop of pressures of 14 ± 5 mm Hg. There was no evidence of bilateral block in 47 cases as evident from contralateral lower limb movements (extension at knee joint). The smaller volumes, low pressures during injections and avoiding medial needle tip direction might have led to unilateral LPBs. In three patients there was a transient severe drop in ABP to 68, 84, and 72mmHg from its original pressures of 150, 164, and 169 systolic which would suggest of an epidural spread. As per assessment in the postoperative period the contralateral limb could be barely moved with patients own efforts confirming an epidural spread. The large volumes of local anesthetics leading to a rapid absorption from the vascular lumbar plexus and the hemisympathectomy can influence the hemodynamics. Cardiac index, invasive arterial blood pressure, and heart rate were measured at baseline and 60 min after lumbar plexus and sciatic block [41]. Cardiac index did not change. There was a significant reduction in mean arterial blood pressure and diastolic blood pressure [41]. The authors concluded LPB and sciatic nerve block did not appear to induce clinically significant hemodynamic changes [41]. The majority of the hemorrhagic complications of a PCB were described in patients receiving anticoagulant or antiplatelet drugs, used for therapeutic indications or thromboprophylaxis. Retroperitoneal hematomas described after a single-injection PCB [42,43]. These patients received anticoagulants after LPBs in the post-operative period. Patients on LMWHs are a contraindication for the blocks in the deeper and vascular areas as in the LPBs. Aidaet al.[44]reported a renal subcapsular hematoma after an L3-PCB. Thus it is prudent to approach the lumbar plexus with the Winnies or the Capdivellas approaches. The inferior renal pole is close to the L3 level, therefore, a lower L4 approach should be safer (Fig. 15).
Dark red arrows – lower poles of kidneys at L2-3 but can extend to L3-4.
Orange line – distance lateral to spinous process.
Blue line – distance from the skin to lumbar plexus.
White brace – distance from the T P to the lumbar plexus.
Green arrow – probable medial spread in the neuraxis.
Level of Evidence
The questions arise whether a combined LPB and SPB that is: ( LSPB ) can be used utilized as sole anesthetic technique for hip surgeries. There are no sufficient studies which establish the role of LSPB as a sole anesthetic technique for the hip surgeries. deVismeet al.[13] described a need for supplement opioids and sedatives for 27% of the patients undergoing hip fracture repair under PCB with an additional SPB. Buckenmaier et al.[45] concluded that a LPB with perineural catheter and sciatic nerve block with perioperative sedation is an effective alternative to general anesthesia for total hip arthroplasty. The variable innervation of the surgical site from the T12 and L1 dermatome is the possible reason for the insufficiency of the LSPB as a sole anesthetic technique for hip surgery [39]. De Leeuwet al. [46] concluded that a paravertebral block of L1 should be considered as an additional technique to overcome the lack of anesthesia in dermatome L1 by a PCB. This author ( S M D ) observed incisional pain ( lateral aspect of thigh ) in more than > 50% patients This author has started advocating and currently studying the role quadratuslumborum block(QLB) in hip patients with 10ml 0.2% ropivacaine as a supplementation to LSPB. QLB provides the subcostal and ilioingiuinal blocks. L1 nerve root block.
Sacral plexus block
Mansour [47] mentioned the point at 6 cm from the PSIS on the line joining the PSIS and the Ischial tuberosity ( IsT). The stimulating needle is inserted perpendicular to the buttock, and after encountering the iliac bone or the sacrum, the needle tip is walked over into the sacral plexus. Clinically, in the event of bone being contacted or failure to elicit a sciatic nerve response, Mansour[47] recommended reinserting the needle more caudally. It is highly important to understand the number of needle passes, as the beyond the bone are is the visceral and vascular structures. In the largest study, a success rate of 94% involving 400 patients was observed in the largest study [49]. In an another study[53] a parasacral plexus block resulted. The parasacral technique reliably blocks the ipsilateral sacral plexus [47,54], has a high success rate (97%) [47,54], and urinary retention is uncommon [47,54]. This author observed a high success rate after its supplementation to the primary LPB. No complications were observed so far in this series. Connor et al.[55] designed a study using healthy volunteers to examine anatomy relevant to the parasacral block. In 3 of 10 volunteers, the MRI simulated needle path encountered small bowel, rectum, and blood vessels/seminal vesicles on first needle pass. Mansour mentions caudal insertion of the needle on bony contact [47]. In the MRI simulation study [55] reinsertion of the simulated needle more caudally did not result in plexus contact. The simulated needle pierced the rectum in one volunteer and perianal fat in three volunteers, suggesting that caudad reinsertion of the needle could be hazardous [55].O’Connor et al.[55] also confirmed that when bone is contacted on the first pass, simply limiting the needle advancement to <2 cm past the bony margin (as recommended) may not be safe as there are intrapelvic structures within reach. Ultrasound can be added advantage to delineate the bony structures the sacral plexus and the pelvic viscera and vascular structures [56]. There are also very few trials evaluating the safety and efficacy of the combination of the two techniques (paravertebral LPB and parasacral sciatic nerve block) [13,22,26,32].Therefore, the true incidence of efficacy as a sole anesthetic technique and its complications are not known. Thus based on published data it appears to be relatively low [13,22,26,32]. Our study adds to the existing study on the techniques and efficacy of the LSPB in high-riskgeriatric fracture hip patients posted for surgical procedures. The uniqueness of this study is all the patients were awake or mildly sedated throughout the surgical procedure and were hemodynamically stable. It was worth to observe the relative-patient immediate interaction in the immediate postoperative period. There were no mortality at the end of one month. These authors will retrospectively study whether the lumbosacral plexus blocks for surgical repair of fracture of intertrochanter are associated with increased survival rates.
Conclusion
Regional anesthesia remains the anesthesia of choice for older and ailing patients [57]. Thus, mode of anesthesia is specifically tailored according to a patient’s requirement at the discretion of the anesthesiologist. Regional anesthesia is associated with a lower odds of inpatient mortality and pulmonary complications among all hip fracture patients compared with general anesthesia. This finding may be driven by a trend toward improved outcomes with regional anesthesia among patients with intertrochanteric fractures [ 58 ]. According to this author the LSPB provides a unique, unilateral and uncomplicated regional anesthesia for the high-risk geriatric patients posted for hip surgeries. The role of ultrasound-guided QLB should be taken into consideration for the incisional pain. This author would like to caution that the LPB is moderately difficult to perform, requires very high vigilance during injection of local anesthetic agent and strict haemodynamic monitoring throughout the surgical period. These authors recommend the Lumbosacral Plexus block as an alternative to the neuraxial blocks in early surgical repair ( < 24-48 hours ) for fracture of intertrochanters in high risk geriartric patients.
References
1. Aharonoff GB, Koval KJ, Skovron ML, Zuckerman JD. Hip fractures in the elderly: Predictors of one year mortality. J Orthop Trauma 1997;11:162-5.
2. Farahmand BY, Michaëlsson K, Ahlbom A, Ljunghall S, Baron JA, Swedish Hip Fracture Study Group.et al. Survival after hip fracture. OsteoporosInt 2005;16:1583-90.
3. Schroder HM, Erlandsen M. Has mortality after a hip fracture increased? J AmGeriatrSoc2007;55:1720-6.
4. Davis FM, Woolner DF, Frampton C,Wilkinson A, Grant A, Harrison RT. Prospective, multicentre trial of mortality following general or spinal anaesthesia for hip surgery in the elderly. Br J Anaesth 1987;59:1080-8
5. Zuckerman ID, Skovron ML, Koval KJ, Aharonoff G, Frankel VH. Postoperative complications and mortality associated with operative delay in older patients who have a fracture of the hip. J Bone Joint Surg Am 1995;77:1-6.
6. Oliver CD, White SA, Platt MW. Surgery for a fractured femur and elective ICU admission at 113 year of age? Br JAnaesth2000;84:260-2.
7. Simunovic N, Devereaux PJ, Sprague S, Guyatt GH, Schemitsch E, Debeer J, et al. Effect of early surgery after hip fracture on mortality and complications: Systematic review and meta-analysis. CMAJ 2010;182:1609-16.
8. Lee DJ, Elfar JC. Timing of hip fracture surgery in the elderly.GeriatrOrthopSurgRehabil 2014;5:138-40.
9. Karaca S,Ayhan E,Kesmezacar H,Uysal O. Hip fracture mortality: Is it affected by anesthesia techniques? Anesthesiol Res Pract2012;2012:708754.
10. Urwin SC, Parker MJ, Griffiths R. General versus regional anaesthesia for hip fracture surgery: A meta-analysis of randomized trials. Br J Anaesth 2000;84:450-5.
11. deVisme V, Picart F, Le Jouan R, Legrand A, Savry C, Morin V, et al. Combined lumbar and sacral plexus block compared with plain bupivacaine spinal anesthesia for hip fractures in the elderly. RegAnesth Pain Med 2000;25:158-62.
12. Chia N, Low TC, Poon KH. Peripheral nerve blocks for lower limb surgery-a choice anaesthetic technique for patients with a recent myocardial infarction?Singapore Med J2002;43:583-6.
13. Ho AM, Karmakar MK. Combined paravertebral lumbar plexus and parasacral sciatic nerve block for reduction of hip fracture in a patient with severe aortic stenosis. Can J Anaesth 2002;49:946-50.
14. Asao Y, Higuchi T, Tsubaki N, Shimoda Y. Combined paravertebral lumbar plexus and parasacral sciatic nerve block for reduction of hip fracture in four patients with severe heart failure. Masui 2005;54:648-52.
15. Naja Z, el Hassan MJ, Khatib H, Ziade MF, Lönnqvist PA. Combined sciatic-paravertebral nerve block vs. General anaesthesia for fractured hip of the elderly. Middle East J Anaesthesiol 2000;15:559-68.
16. Fanelli G, Casati A, Aldegheri G, Beccaria P, Berti M, Leoni A, et al. Cardiovascular effects of two different regional anaesthetic techniques for unilateral leg surgery. ActaAnaesthesiolScand 1998;42:80-4.
17. Stevens RD, Van Gessel E, Flory N, Fournier R, Gamulin Z. Lumbar plexus block reduces pain and blood loss associated with total hip arthroplasty. Anesthesiology 2000;93:115-21.
18. Birnbaum K, Prescher A, Hessler S, Heller KD. The sensory innervation of the hip joint – An anatomical study. SurgRadiolAnat 1997;19:371-5.
19. Farny J, Girard M, Drolet P. Posterior approach to the lumbar plexus combined with a sciatic nerve block using lidocaine. Can J Anaesth 1994;41:486-91.
20. Ripart J, Cuvillon P, Nouvellon E, Gaertner E, Eledjam JJ. Parasacral approach to block the sciatic nerve: A 400-case survey. RegAnesth Pain Med 2005;30:193-7.
21. Capdevila X, Macaire P, Dadure C, Choquet O, Biboulet P, Ryckwaert Y, et al. Continuous psoas compartment block for postoperative analgesia after total hip arthroplasty: New landmarks, technical guidelines, and clinical evaluation. AnesthAnalg 2002;94:1606-13.
22. Mannion S, Barrett J, Kelly D, Murphy DB, Shorten GD. A description of the spread of injectate after psoas compartment block using magnetic resonance imaging. RegAnesth Pain Med 2005;30:567-71.
23. Parkinson SK, Mueller JB, Little WL, Bailey SL.Extent of blockade with various approaches to the lumbar plexus.AnesthAnalg1989;68:243-8.
24. O’Callaghan S, Walsh M, Murphy DB, and Shorten GD. In with the new, out with the old? Comparison of two approaches for psoas compartment blockStephen Mannion.AnesthAnalg 2005;101:259-64.
25. Dalens B, Tanguy A, Vanneuville G. Lumbar plexus block in children: A comparison of two procedures in 50 patients. AnesthAnalg 1988;67:750-8.
26. Karmakar MK, Ho AM, Li X, Kwok WH, Tsang K, NganKee WD, et al. Ultrasound-guided lumbar plexus block through the acoustic window of the lumbar ultrasound trident. Br J Anaesth 2008;100:533-7.
27. Gadsden JC, Lindenmuth DM, Hadzic A, Xu D, Somasundarum L, Flisinski KA, et al. Lumbar plexus block using high-pressure injection leads to contralateral and epidural spread. Anesthesiology 2008;109:683-8.
28. Mannion S.Psoas compartment block. ContinEducAnaesthCrit Care Pain 2007;7:162-6.
29. deLeeuw MA, Slagt C, Hoeksema M, Zuurmond WW, Perez RS. Hemodynamic changes during a combined psoas compartment-sciatic nerve block for elective orthopedic surgery. AnesthAnalg 2011;112:719-24.
30. Weller RS, Gerancher JC, Crews JC, Wade KL. Extensive retroperitoneal hematoma without neurologic deficit in two patients who underwent lumbar plexus block and were later anticoagulated. Anesthesiology 2003;98:581-5.
31. AvelineC, Bonnet F.Delayed retroperitoneal haematoma after failed lumbar plexus block. Br JAnaesth2004;93:589-91.
32. Aida S, Takahashi H, Shimoji K. Renal sub capsular hematoma after lumbar plexus block. Anesthesiology 1996;84:452-5.
33. Buckenmaier CC 3rd, Xenos JS, Nilsen SM. Lumbar plexus block with perineural catheter and sciatic nerve block for total hip arthroplasty. J Arthroplasty 2002;17:499-502.
34. deLeeuw MA, Dertinger JA, Hulshoff L, Hoeksema M, Perez RS, Zuurmond WW, et al. The efficacy of levobupivacaine, ropivacaine, and bupivacaine for combined psoas compartment-sciatic nerve block in patients undergoing total hip arthroplasty. Pain Pract 2008;8:241-7.
35. Mansour NY. Re-evaluating the sciatic nerve block: Another landmark for consideration. RegAnesth 1993;18:322-3.
36. Berry M, Bannister LH, Standring SM. Nervous system. In: Williams PL, editor. Gray’s Anatomy. 38thed. New York: Churchill Livingstone; 1995. p. 1277-82.
37. Ripart J, Cuvillon P, Nouvellon E, Gaertner E, Eledjam JJ. Parasacral approach to block the sciatic nerve: A 400-case survey. RegAnesth Pain Med 2005;30:193-7.
38. Bailey SL, Parkinson SK, Little WL, Simmerman SR. Sciatic nerve block. A comparison of single versus double injection technique. RegAnesth 1994;19:9-13.
39. Fanelli G, Casati A, Garancini P, Torri G. Nerve stimulator and multiple injection technique for upper and lower limb blockade: Failure rate, patient acceptance, and neurologic complications. Study group on regional anesthesia. AnesthAnalg 1999;88:847-52.
40. Jochum D, Iohom G, Choquet O, Macalou D, Ouologuem S, Meuret P, et al. Adding a selective obturator nerve block to the parasacral sciatic nerve block: An evaluation. AnesthAnalg 2004;99:1544-9.
41. Cuvillon P, Ripart J, Jeannes P, Mahamat A, Boisson C, L’Hermite J, et al. Comparison of the parasacral approach and the posterior approach, with single-and double-injection techniques, to block the sciatic nerve. Anesthesiology 2003;98:1436-41.
42. Morris GF, Lang SA, Dust WN, Van der Wal M. The parasacral sciatic nerve block. RegAnesth 1997;22:223-8.
43. O’Connor M, Coleman M, Wallis F, Harmon D. An anatomical study of the parasacral block using magnetic resonance imaging of healthy volunteers. AnesthAnalg 2009;108:1708-12.
44. Bendtsen TF, Lönnqvist PA, JepsenKV, Petersen M, Knudsen L, Børglum J, et al. Preliminary results of a new ultrasound-guided approach to block the sacral plexus: The parasacral parallel shift. Br J Anaesth 2011;107:278-80.
45. Beaupre LA, Jones CA, Saunders LD, Johnston DWC, Buckingham J, Majumdar SR. Best practices for elderly hip fracture patients: a systematic overview of the evidence. Journal of General Internal Medicine. 2005;20(11):1019–1025.
58. Neuman MD, Silber JH, Elkassabany NM, Ludwig JM, Fleisher LA. Comparative effectiveness of regional versus general anesthesia for hip fracture surgery in adults. Anesthesiology. 2012 Jul;117(1):72-92.
| How to Cite this Article: Diwan S, Pradhan C, Patil A, Puram C, Sancheti P. Combined lumbar and sacral plexus block in geriatric high-risk patients undergoing an awake repair of fracture intertrochanteric of femur. Journal of Anaesthesia and Critical Care Case Reports Jan-April 2018; 4(1):21-30. |