Vol 3 | Issue 1 | Jan-Apr 2017 | page: 8-10 | Patrick Thomas Thorburn, Jonathan Hyde, Siobhan Dallibar, Nigel Marchbank, Nevil Hutchinson, Soraya Conroy, Michael Lewis
Authors: Patrick Thomas Thorburn [1], Jonathan Hyde [1], Siobhan Dallibar [1], Nigel Marchbank [1], Nevil Hutchinson [1], Soraya Conroy [1], Michael Lewis [1]
[1] Brighton and Sussex University Hospitals NHS Trust, United Kingdom.
Address of Correspondence
Dr. Patrick Thomas Thorburn
Brighton and Sussex University Hospitals NHS
Trust, United Kingdom
Email: P.t.thorburn@gmail.com
Abstract
Introduction: Minimally invasive video-assisted thoracoscopic surgery (VATS) is a technique that is increasingly
employed for atrial fibrillation (AF) ablation. There is a growing body of evidence that surgical ablation using VATS is superior to traditional catheter ablation. However, the procedure is associated with serious complications including midline sternotomy for bleeding, pacemaker requirement, pneumothorax, haemothorax, stroke, tamponade and rib fracture. We present details of a previously undescribed complication of acute cardiac herniation following VATS ablation.
Case Report: A 35-year-old male security guard was diagnosed with AF in August 2011. After failing to respond to medical therapy, he was referred for VATS ablation and left atrial appendage occlusion. The procedure was successful but the patient deteriorated in the intensive care unit. He became hypotensive (88/40mmHg) and tachycardic (120bpm) with intermittent episodes of bradycardia (<60bpm). He was profoundly clammy with a reduced capillary refill time and consciousness level. Despite fluid boluses and vasopressors, he remained critically unwell. Chest X-Ray revealed acute cardiac herniation and he quickly returned to theatre for correction.
Conclusion: This case-study highlights an extremely rare, but life-threatening complication associated with VATS ablation – acute cardiac herniation though the open right pericardium. To our knowledge, this has not previously been described and has prompted us to change our own practice. We now electively close the pericardium in all VATS ablation cases. Early recognition of the clinical signs and chest X-Ray findings associated with acute cardiac herniation could be life-saving.
Keywords: Video-assisted thoracoscopic surgery (VATS), atrial fibrillation (AF), surgical ablation, acute cardiac herniation, acute dextrocardia.
Introduction
Minimally invasive video-assisted thoracoscopic surgery (VATS) is a technique that is increasingly employed for atrial fibrillation (AF) ablation. Radiofrequency or cryoablation is applied directly to the epicardium through a bilateral approach (occasionally unilateral). Some case series report 65% -81% patients remain free from AF at 12 months [1,2]. A recent randomised controlled trial (RCT) has shown that surgical ablation (SA) performed by VATS under general anaesthesia is superior to catheter ablation (CA). They reported freedom from left atrial (LA) arrhythmia without the need for anti-arrhythmic drugs of 36.5% (CA) vs. 65.6% in (VATS) [3]. The study population was limited to those with dilated LA or failed previous CA. However, the authors noted a significantly increased procedural adverse event rate of 24% (SA) vs. 3.2% (CA). Complications included; midline sternotomy for bleeding, pacemaker requirement, pneumothorax, haemothorax, stroke, tamponade and rib fracture. We present details of a previously undescribed complication of cardiac herniation following VATS ablation in an otherwise fit 35-year-old male.
Case Report
A 35-year-old male security guard was diagnosed with AF in August 2011. He underwent successful DC cardioversion in April 2013 but relapsed to persistent AF in June 2014. After failing to respond to medical therapy, he was referred for VATS ablation and left atrial appendage (LAA) occlusion.
The procedure was performed under general anaesthesia with a left-sided double-lumen tube and standard monitoring supplemented with invasive arterial blood pressure monitoring and right-sided internal jugular vein cannula. VATS ablation was performed through a bilateral (right side first) approach as described by Yilmaz et al. [4] using the AtriCureâ endoclamp and monopolar pen. The pericardium was opened on each side for access but was not subsequently closed: this has been our technique for over 50 cases. Ablation (with LAA occlusion) led to clinical termination of AF and return to sinus rhythm in the operating room. Analgesia was provided with 2g intravenous (IV) paracetamol, 75mg IV diclofenac, 10mg IV morphine and 40ml 0.25% L-bupivicaine for intercostal nerve blocks and port site infiltration on both sides. At the end of the procedure, the patient was haemodynamically stable and was shifted to cardiac ITU for ongoing care after extubation.
Soon after arrival in ITU his clinical condition deteriorated. He became hypotensive (88/40mmHg) and tachycardic (120bpm) with intermittent episodes of bradycardia (<60bpm). He was profoundly clammy with a reduced capillary refill time and consciousness level. There was evidence of venous congestion with significant engorgement of the neck veins, facial cyanosis and a high central venous pressure. He remained hypotensive despite repeated boluses of fluid and metaraminol.
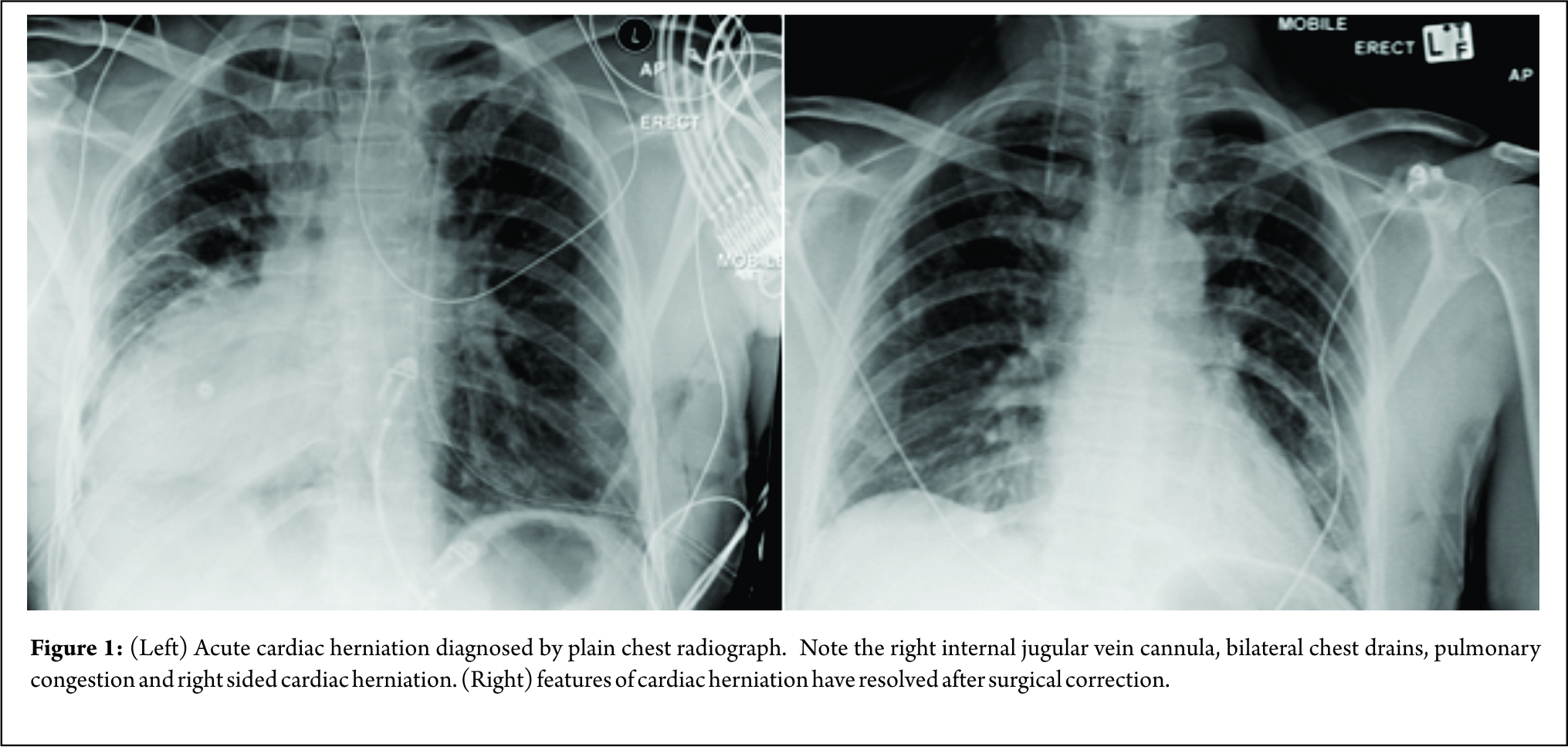
The cause of his acutely unstable condition remained unclear until a portable antero-posterior chest X-ray (CXR) was performed (Fig 1). When the image was initially reviewed at the bedside, it was flipped to place the cardiac shadow on the left side by the clinical team. However,the ECG lead orientation confirmed that the heart was on the right and acute cardiac herniation was diagnosed following discussion with a chest radiologist. The patient was transferred expeditiously back to the anaesthetic room whilst the operating theatre was prepared. He was maintained in a ‘right side up’ position resulting in an improvement in his clinical condition: mentation returned to normal and he felt better. The heart rate stabilised and blood pressure improved.
Anaesthesia was induced in the operating room while the patient was subsequently prepared and draped. Anaesthetic and surgical teams were scrubbed and ready for two eventualities: (1) haemodynamic instability following induction, in which case a midline sternotomy would be performed; or (2) clinical stability, in which case thoracoscopic reduction of the cardiac herniation would be attempted.
After induction of anaesthesia the patient’s condition remained stable. An oral endo-tracheal tube was placed with a right-sided bronchial blocker. The right lung was deflated without any clinical compromise and the thoracoscope and instruments were inserted with caution through the original right-sided port sites. On careful digital insertion through the upper port, the left ventricle was found to be pressed up against the inner aspect of the chest wall. Using the blunt-tipped, soft pool-suction catheter as a lever between the heart and the chest wall, the herniated heart was carefully reduced back into the pericardium. Clinical stability was maintained throughout the procedure. The pericardium was then closed using two sutures to prevent recurrence.
The patient returned to the cardiac ITU where he was ventilated overnight and extubated successfully the following morning. Post- extubation CXR (Fig 1) shows return of the heart to the left side. He remained in sinus rhythm throughout his hospital stay and was discharged home 72 hours after the initial procedure, having had this rare complication explained to him.
Discussion
Cardiac herniation was first documented by Bettman and Tennenbaum in 1948 [5] and has since been described in patients with traumatic and iatrogenic defects to their pericardium [6,7]. As a surgical complication it is most commonly recognised in pneumonectomy with deliberate breach of the pericardium and the incidence can be as high as 3% in extra-pleural pneumonectomy following chemotherapy [8]. To our knowledge it has not been described in the literature following VATS ablation for AF. Right sided cardiac herniation causes torsion of the great vessels resulting in reduction of venous return and obstruction to cardiac output. Mortality is high at around 50-100%, although clinical presentation varies widely, with some patients being asymptomatic [9].
In this case-study, the plain CXR was essential in making the diagnosis underlining the importance of a CXR in patients with acute deterioration following thoracic surgery. The most likely diagnosis at the time the CXR was taken was bleeding. An initial clinical review assumed that the CXR had been transposed, rather than that the CXR was correctly marked. The case highlights the importance of multi-disciplinary working in the hospital environment; a culture entrenched in surgical practice largely due to the success of the World Health Organisation surgical checklist.
Conclusion
This case report highlights an extremely rare, but life-threatening complication associated with VATS ablation for AF – acute cardiac herniation though the open right pericardium. To our knowledge this has not previously been described.
The case has prompted us to change our own practice and we now electively close the pericardium in all VATS ablation cases. In writing this report we hope to increase awareness of cardiac herniation as a potential cause for post-operative haemodynamic instability in situations where the pericardium on the right side has been opened but not closed. We also want to highlight the value of engaging the multi-disciplinary team in a crisis. It was the radiographer who identified the CXR was orientated correctly. It was these radiological findings coupled with the clinical signs that allowed early recognition of acute cardiac herniation and life-saving intervention.
References
1. Han FT, Kasirajan V, Kowalski M, et al. Results of a minimally invasive surgical pulmonary vein isolation and ganglionic plexi ablation for atrial fibrillation: single-center experience with 12-month follow-up. Circ Arrhythm Electrophysiol 2009;2:370-7
2. Edgerton JR, Brinkman WT, Weaver T, et al. Pulmonary vein isolation and autonomic denervation for the management of paroxysmal atrial fibrillation by a minimally invasive surgical approach. J Thorac Cardiovasc Surg 2010;140:823-8
3. Boersma LV, Castella M, Van Boven WJ, Berruezo A, et al. Atrial Fibrillation Catheter Ablation Versus Surgical Ablation Treatment (FAST): A 2-Center Randomized Clinical Trial. Circulation. 2012;125:23-30.
4. Yilmaz A, Geuzebroek GS, Van Putte BP, Boersma LV, et al. Completely thoracoscopic pulmonary vein isolation with ganglionic plexus ablation and left atrial appendage amputation for treatment of atrial fibrillation. Eur J Cardiothorac Surg. 2010;38(3):356–360
5. Bettman BB, Tannenbaum WJ. Herniation of the heart through a peri- cardial incision. Ann Surg 1948;128:1012–1014.
6. Schir F, Thony F, Chavanon O, Perez-Moreira I, et al. Blunt traumatic rupture of the pericardium with cardiac herniation: two cases diagnosed using computed tomography. Eur Radiol 2001;11:995–999.
7. Mehanna MJ, Israel GM, Katigbak M, Rubinowitz AN. Cardiac herniation after right pneumonectomy. Case report and review of the literature. J Thorac Imaging 2007;22:280–282.
8. Opitz I, Kestenholz P, Lardinois D, Muller M, et al. Incidence and management of complications after neoadjuvant chemotherapy followed by extrapleural pneumonectomy for malignant pleural mesothelioma. Eur J Cardiothorac Surg 2006;29:579–584.
9. Kawamukai K., Antonacci F., Di Saverio S. and Boaron M. Acute postoperative cardiac herniation. Interactive cardiovascular and thoracic surgery 2011;12(1):73-74.
| How to Cite this Article: Thorburn PT, Hyde J, Dallibar S, Marchbank N, Hutchinson N, Conroy S, Lewis M. Acute Cardiac Herniation – A Rare Complication of Video-assisted Thoracoscopic Surgery for Atrial Fibrillation. Journal of Anaesthesia and Critical Care Case Reports Jan-Apr 2017; 3(1):8-10. |
