Vol 5 | Issue 1 | Jan-April 2019 | page: 11-13 | Sunil Malik, Shiv Kumar Singh
Authors: Sunil Malik [1], Shiv Kumar Singh [2].
[1] Department of Anesthesiology, Manipal Hospitals, Dwarka, New Delhi, India.
[2] Department of Anaesthesia 11th Floor, Royal Liverpool University Hospital, Prescot Street, Liverpool L7 8XP, UK.
Address of Correspondence
Dr. Sunil Malik,
DNB, B-33 Vishal Enclave, New Delhi 110027, India
E-Mail: drsunilmalik@yahoo.co.in
Abstract
Objective: Managing Post Dural Puncture Headache (PDPH) is a challenge for most anesthesiologist as the gold standard, epidural blood patch (EBP) itself can lead to Dural Puncture that caused the complication in the first place. Medical management of PDPH may not provide symptomatic relief and anesthesiologists are on a constant lookout for techniques that can provide instant and sustained relief from this debilitating complication. Sphenopalatine Ganglion (SPG) and Greater Occipital Nerve (GON) Block have been used individually to manage PDPH in a selected number of patients. For the first time in the literature, we propose the use of a less invasive and acceptable technique using both these blocks (combined nerve and ganglion block) in the same patient to provide higher success rates. The hypothesis for this NAG Dual Block is because both these blocks act on two important but different paths in the pathogenesis of PDPH. In this case series, we describe our experience in 7 patients with PDPH who consented for the dual block.
Case Series: We describe the successful use of NAG dual block in seven patients with PDPH who had immediate and sustained relief. The patients were followed up for up to 48hrs.
Conclusions: We recommend combining both the blocks that are less invasive than EBP for managing PDPH. The Superiority of this new technique will need more data either by RCTs or larger case series. Along with ongoing supportive medical management, both these blocks can be offered as a rescue to all patients diagnosed with moderate to severe PDPH.
Keywords: NAG (Nerve And Ganglion), Post Dural Puncture Headache (PDPH), Greater Occipital Nerve (GON), Sphenopalatine Ganglion (SPG).
Introduction
Management of Post Dural Puncture Headache (PDPH) has always been challenging for anesthesiologists. PDPH not only increases the misery of the patient, but it also prevents bonding with the newborn and increases the length of stay. Economically, it increases the overall cost of treatment. Although the Epidural Blood Patch (EBP) is considered the gold standard and an effective way of managing the problem, the procedure can itself lead to another inadvertent Dural Puncture (D P). Inrecenty ears, Sphenopalatine Ganglion Block [1] or Greater Occipital Nerve Block [2] have been individually used successfully to manage PDPH in a selected number of patients. For the first time in the literature, we propose the use of both these blocks (combined nerve and ganglion block) in the same patient providing higher success. The hypothesis for this NAG Dual Block is because both these blocks act on two important but different paths inthe pathogenesis of PDPH. Further prospective studies will be able to establish the efficacy and effectiveness of NAG dual blocks. Patients would be greatly benefited by this lesser invasive technique due to early recovery and lesser suffering. In this case series, we describe our experience in 7 patients with PDPH who consented for the dual block.
Case Report
Methodology
Over the last two years, we observed 7 patients with PDPH after accidental Dural Puncture. Following failed conservative therapy in these 7 patients, we provided options of combined Greater Occipital Nerve Block (GONB) and Sphenopalatine Ganglion Block (SPB) i.e. NAG dual block or Epidural Blood Patch (EBP) to these patients. All the 7 patients opted for the dual block which would be followed by EBP in case of failure of treatment. Neurologist’s opinion was sought in all the 7 patients to rule out any other cause for the headache. Patients with any neurological deficit would be excluded from the treatment. Patients have explained the procedure in details and informed verbal consent for the dual blocks was obtained.
Block Description
The blocks were performed bilaterally in all the patients. Single anesthetist (1st author) performed all the blocks maintaining uniformity of technique. In all cases, minimum standard monitoring was established, and intravenous access obtained before performing the block under aseptic conditions.
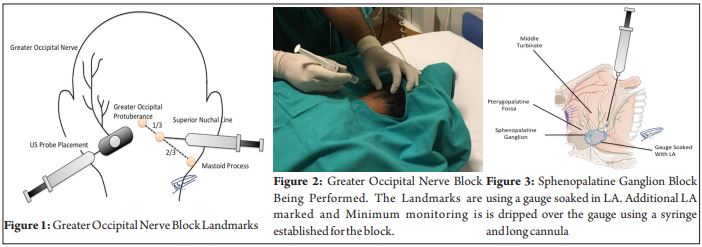
Greater Occipital Nerve (GON) Block
The Patient is positioned prone with a pillow under the chest. Occipital protuberance and mastoid process are marked. A line is drawn connecting the two points. The connecting line is then divided into three parts. The junction of medial 1/3 with the lateral 2/3 corresponds to the point where the GON is blocked (junction of medial 2/3 and lateral 1/3 corresponds to the lesser occipital nerve). 2ml of 0.25% Bupivacaine mixed with 2ml of 2% preservative-free lignocaine wa s mix ed to be us ed a s the loc a l anaesthetics. 1-1.5 ml of this was injected bilaterally at GON landmark after palpating a greater occipital artery and injected just medial to it after careful aspiration. Ultrasound assistance was taken if arterial pulsation was not appreciated. The Patient was monitored for 5mins in the same position before turning supine to look for any swelling or hematoma at the site of injection.
Sphenopalatine ganglion (SPG) block
Patient lies supine with a pillow placed under the scapular area so that the neck is extended providing sniffing position. A gauge piece soaked with 4% lignocaine 2ml is gently inserted into each nostril till it meets resistance. Another 0.5 ml of 4% lignocaine is trickled using a syringe and cannula until the patient feels the drug dripping at the back of the throat. Patient is then maintained in this position for 10 minutes and the nasal packs a re removed. Pati ent is monitored throughout the procedure The local site of the greater occipital nerve block done earlier is again examined for any swelling and hematoma and the nasal passage is examined for any bleed. Patient is monitored for an hour before allowing them to walk to assess the persistence of the symptoms. Inpatients were sent back to the ward after about 2 hours and the outpatients were discharged in similar time scales.All patients were prescribed a combination of Paracetamol 650mg and Caffeine 35mg to be taken regularly three times a day for a further 3 days. They were followed up on phone after 24hrs and at 48hrs. An outpatient visit was arranged after one week to assess for any side effects and recurrence of headache. Further, follow-upswere done on phone thereafter.
Results
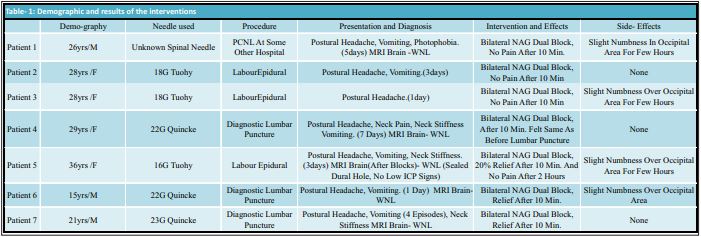
All the 7 patients received both bilateral SPB and GONB (Table-1). Monitored for one hour for any side effects in the hospital. Pain and other symptoms (nausea, vomiting, photophobia) started subsiding within 10 minutes of administration of the block in all the patients. By the time of discharge or shifting back to the ward after two hours, headache and other symptoms had completely subsided and there were no side effects apart from little numbness in an occipital area in most of the patients. Follow up done on phone after 24 and 48hrs and outpatient visit after one week and on phone thereafter. MRI (pre-blocks) was done in 3 patients (2 patients of diagnostic lumbar puncture and 1 patient of multiple spinal attempts) to rule out any other cause of headache and signs of altered ICP. MRI (after blocks)was done in one labour epidural (16G Tuohy needle was used) patient to rule out persistent CSF leak and altered ICP to plan a safe discharge from hospital. No neurological deficit was found in any patient before and after the blocks.
Discussion
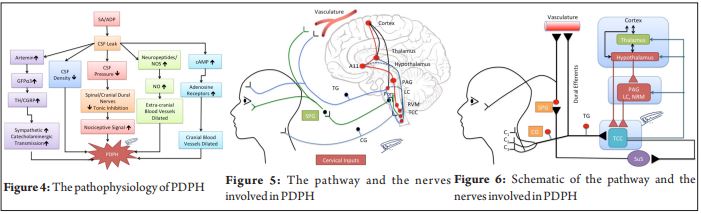
The occurrence of PDPH has its own pathological bases. For the cranial innervations, studies have shown that the dura mater is heavily innervated and most likely cause of the intense pain [3]. Activation of the intracranial nerves and abnormal distention of the extracerebral blood vessels can consequently activate the trigeminal nervous system that was thought to be the origins of headache [4]. Studies proposed that a tonic inhibition of the spinal and Cranial Dural nerves exists under normal CSF pressure, but this inhibition would be reduced or reversely activated by a chronic leakage of CSF after lumbar puncture [5], [Fig- 4,5 and 6]. The rationale for using greater occipital nerve block comes from the proximity of sensory neurons in the upper cervical spinal cord to the Trigeminal Nucleus Caudalis (TNC) neurons and the convergence of sensory input to TNC neurons from both cervical and trigeminal fibers [6] and GONB decreases this nociceptive signal maintaining this tonic inhibition. Since the first case has been reported on the successful treatment of PDPH with a greater occipital nerve block (GONB) [7], several other PDPH patients from different institutes were presented after treatment with GONB [8].Another hypothesis for PDPH is cerebral and extracerebral venous dilatation. Cerebral vasodilatation is responsible for the excruciating headache after a Dural Puncture. One of the contributors to this vasodilatation ismediated by parasympathetic activity by the neurons which have synapses in the SPG. This is how an SPG block helps in alleviating the headache that is mediated by the neurons in the SPG [ 9 ]. Intr ana s a l l idoc a ine admin istration anesthetizes the sphenopalatine ganglion and decreases the nociceptor signaling, which relieves the PDPH[10]. CSF l e a k age a lthough considered as a main cause but it is still unclear as the cause, physiologically, the CSF loss is rapidly compensated by rapid turnover. Challenges to epidural blood patch (EBP) exist as it has absolute and relative contraindications; persistent pain despite EBP, high complication rates. Sealing mechanism is still controversial as evidenced by EBP done at a lumbar level providing relief for PDPH from the cervical tap[11]. In one of our patient ( no.5 table- 1) who suffered two dural punctures with 16G Tuohy needle, the holes were found sealed with no signs of low ICP after 4 days on MRI scan, suggesting self-sealing.
Conclusion
We for the first time propose utilizing combined bilaterally GONB and SPB (NAG DUAL BLOCK) instead of doing just one of them. The dual block targets the different important steps in the pathogenesis of PDPH prov iding much higher success rate compared to utilizing the individual blocks. They appear to be simple, minimally invasive blocks that can be done as bedside procedures. If successful, invasive procedure like EBP does not need to be done despite it being an established modality with a high success rate for managing PDPH. The data on doing these blocks individually for PDPH is scarce now and there is no data on combined blocks yet. Publications on the efficacy of the SPB and GONB individually by several approaches for headaches of varied etiology have proven their worth. We recommend combining both the blocks that are less invasive than EBP for managing PDPH. Before declaring the superiority of the NAG dual block over the time tested EBP, we need to have more data on successfully treated patients. After reviewing the available literature, it appears that we should routinely offer both the blocks to all patients diagnosed with moderate to severe PDPH before an invasive procedure like EBP. If the NAG dual block is ineffective in alleviating pain, EBP can then be offered to the patient. Clinicians should continue ongoing supportive medical management after performing the blocks.
References
1. Cohen S, Sakr A, Katyal S, Chopra D. Sphenopalatine ganglion block for postdural puncture headache. Anaesthesia. 2009;64:574–575.
2. Niraj, G. et al. Greater occipital nerve block for postdural puncture headache (PDPH): A prospective audit of a modified guideline for the management of PDPH and review of the literature.Journal of Clinical Anesthesia, Volume 26, Issue 7, 539 – 544.
3. Kemp WJ III, Tubbs RS, Cohen-Gadol AA. The innervation of the cranial dura mater: neurosurgical case correlates and a review of the literature. World Neurosurgery 2012;78(5) 505-510.
4. Cumberbatch MJ, Williamson DJ, Mason GS, Hill RG, Hargreaves RJ. Dural vasodilation causes a sensitization of rat caudal trigeminal neurons in vivo that is blocked by a 5-HT1B/1D agonist. British Journal of Pharmacology 1999;126(6) 1478-1486.
5. Fuzhou Wang (July 10th 2014). Post Dural Puncture Headache – We Can Prevent It, Pain and Treatment Gabor Racz, Intech Open, DOI: 10.5772/57408
6. Ashkenazi A, Levin M. Greater occipital nerve block for migraine and other headaches: is it useful? Current Pain and Headache Reports 2007; 11: 231–5.
7. Matute E, Bonilla S, Gironés A, Planas A. Bilateral greater occipital nerve block for post-dural puncture headache. Anaesthesia 2008;63(5) 557-558.
8. Akin Takmaz S, UnalKantekin C, Kaymak C, Başar H. Treatment of post-dural puncture headache with bilateral greater occipital nerve block. Headache 2010;50(5) 869-872.
9. Piagkou M, Demesticha T, Troupis T, Vlasis K, Skandalakis P, Makri A, et al. The pterygopalatine ganglion and its role in various pain syndromes: from anatomy to clinical practice. Pain Pract 2012; 12: 399-412.
10. Robbins MS, Robertson CE, Kaplan E, et al. The sphenopalatine ganglion: anatomy, pathophysiology, and therapeutic targeting in headache. Headache. 2016; 56:240–258.
11. Lebrun C, Peek D, Vanelderen P, Van ZundertJ.Unintentional cervical dural tap treated with lumbar blood patch. PainPract. 2014 Jul;14(6):577-80.
| How to Cite this Article: Malik S, Singh S K. A Novel NAG (Nerve And Ganglion) Dual Block For PDPH: An Observational Study In Seven Patients Of Refractory Post Dural Puncture Headache (PDPH) Using Combined Greater Occipital Nerve (GON) And Sphenopalatine Ganglion (SPG) Blocks. Journal of Anaesthesia and Critical Care Case Reports Jan-April 2019;5(1):14-17. |

(Full Text HTML) (Download PDF)
.