Vol 5 | Issue 3 | Sep-Dec 2019 | page: 10-12 | Astha Agrawal Kanaparthi , Vikas Nair , Pramod Kale , Arvind Kate
Authors: Astha Agrawal Kanaparthi [1] , Vikas Nair [1] , Pramod Kale [1] , Arvind Kate [2]
Address of Correspondence
1Department of Anesthesiology, Zen Multi Specialty Hospital, Chembur, Mumbai, India.
2Department of TB & Respiratory Medicine, Zen Multi Specialty Hospital, Chembur, Mumbai, India.
Dr. Astha Agrawal Kanaparthi
Zen Multi Specialty Hospital, Chembur, Mumbai, India
Email: astha2087@gmail.com
Abstract
Introduction: Bronchoscopy is performed for diagnostic and therapeutic purposes. It is a challenge for the anaesthesiologist to maintain ventilation for the patient as the patients’ airway is shared between the anaesthetist and the bronchoscopist. Many modalities have been used for anaesthesia and airway management for bronchoscopies. We present a case of bronchoscopy guided foreign body removal under anaesthesia. Spontaneous ventilation was maintained in the patient with the help of nasal airways.
Keywords: Bronchoscopy, Ventilation, Nasal airway.
Introduction
Bronchoscopy is defined as an endoscopic technique of visualizing the inside of the airways for diagnostic and therapeutic purposes. A bronchoscope is inserted into the airways, usually through the nose or mouth, or oc c a siona l l y through a tracheostomy. Bronchoscopy can be used for diagnostic or therapeutic procedures. Therapeutic bronchoscopies require more time and greater depth of anaesthesia to prevent sudden movement of the patient. It is a challenge for the anaesthesiologist to maintain ventilation during prolonged bronchoscopic procedures as the airway is shared with the bronchoscopist. Various methods of airway management have been used to maintain a patent airway, ranging from nasal cannula to supraglottic devices like laryngeal mask airway to a n endotracheal tube. Choosing the most adequate method, considering the pathology and site of the lesion, the interventional procedure and the possible risks is important [1, 2]. A nasopharyngeal airway is a simple device that can be conveniently inserted into the supraglottic airway to secure an open passage [3]. According to the 2010 American Heart Association Guide lines for Cardiopulmonar y Resuscitation and Emergenc y Cardiova scular Care, a supraglottic airway device (not tracheal intubation) should be the first choice used during emergent resuscitation. The nasopharyngeal airway is an example of a supraglottic airway device used for such conditions [4]. We present a case of bronchoscopic removal of foreign body from the lung. Bilateral nasal airways were used to maintain the ventilation.
Case Report
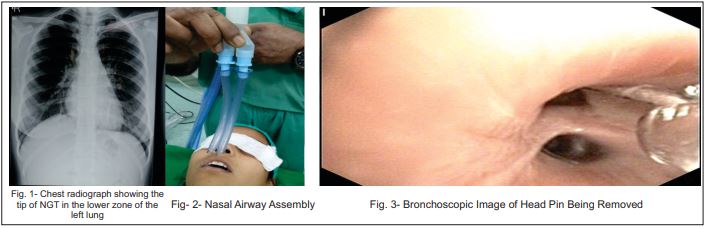
An 18 year old girl with out any comorbidities was referred to our hospital with a history of accidental aspiration of a sharp head pin. She had a failed attempt at bronchoscopic removal elsewhere and was advised left lobectomy there. She had no presenting complaints. On X-Ray and CT scan, the head pin was visualised in the left lower lobe of the lung. Urgent removal of the pin was necessary as there was a risk of injury to the surrounding tissue. The aim was to ensure easy removal of the pin without any dislodgement or injury to surrounding structures without any discomfort to the pati ent. Afte r dis cussing with the pulmonologist performing the procedure, it was decided to perform flexible bronchoscopy through trans-oral route with ventilation through bilateral nasal airways.All routine preoperative investigations were normal. Adequate starvation was confirmed and appropriate consent was taken from the patient and her parents. Nebulization with four percent lignocaine was given 20 minutes before starting the procedure. ECG, pulse oximeter and non-invasive blood pressure were attached and monitored throughout the procedure. A 20 G IV access was secured and Ringer Lactate was started. The patient was premedicated with injection of Glycopyrolate 0.2mg, injection Midazolam 0.05mg/kg and injection Fentanyl 2mcg/kg. After inducing the patient with 1mg/kg of injection Propofol, Size seven silicon nasal airways were inserted, one in each nostril. The size of the airway to be used was decided by ex amining the outer diameter of nasopharyngeal airway lumen and patients’ nostrils. An adequate sized airway reaches from the patients’ nostril to the angle of the jaw. The surface of the airway was lubricated with lidocaine gel before insertion. The curved end of the airway was inverted towards the hard palate or the roof of the mouth and pl aced at the posterior nasopharynx till the flared end was against the nostril. Both the airways were connected to the Y piece of a double lumen tube with the help of universal connectors and further connected to the anaesthesia circuit. Patient was maintained on air and oxygen. Anaesthesia was maintained with titrated infusions of Propofol 3-5mcg/kg/min and Dexmedetomidine 0.4-0.7mcg/kg/hour. ETCO2 was monitored throughout the procedure. Patient continued to breathe spontaneously as seen by the ETCO2 graph and movement of the bag. The bronchoscope was introduced through the trans-oral route with the help of a bite block which was inserted be fore admin istration of anaesthesia. There was no need to disconnect the circuit for inserting the bronchoscope. Four percent lignocaine was sprayed on the vocal cords through the bronchoscope channel two minutes before introducing it through the vocal cords. After bronchoscopic visualisation of the pin in the left lower lobe, it was grasped with Rat tooth forceps and removed with slow with drawa lofbronchoscope through oral route. The procedure took around 30 minutes. The pin was removed safely and there was no injury to bronchial tree. Patient was hemodynamically stable throughout the procedure and saturation was maintained above 93% throughout. After the procedure, when the patient was awake, the nasal airways were removed carefully. There was no injury to the nasal cavity. The patient was monitored in the recovery room with oxygen on 4 lit/min by face mask till she was fully awake.
Discussion
Fibreoptic bronchoscopy is commonly used for the diagnosis and management of a variety of lung diseases [5, 6]. Desaturation during the procedure is common and requires saturation monitoring and, when needed, oxygen supplementation [6, 7]. A patient who undergoes bronchoscopy frequently suffers pain, cough and a sensation of asphyxiation. They might remember the procedure as a disagreeable experience [8]. The control of coughing is of paramount importance for the quality of bronchoscopy, as this facilitates ease of viewing the bronchial tree. Excessive cough can substantially increase the risk of complications and difficulty in performance of bronchoscopy especially during invasive procedures. Sedation is therefore strongly recommended in order to reduce the stress reaction, enhance patient cooperation, diminish the levels of anxiety and fear, provide amnesia and prevent coughing during the intervention [8]. For therapeutic bronchoscopic procedures, such as prolonged laser therapy, endobronchial sonography, stent implantation (usually with rigid instruments), embedded foreign body as in our case, general anaesthesia is necessary [9]. General anaesthesia is also necessary in children, restless or agitated adults. Supraglottic devices usually laryngeal mask airway have been used for bronchoscopy since 1982. The LMA was found to be beneficial in operator view, flexibility, and also in maintaining stable oxygen saturation [6]. However it occupies the oral cavity and removal of foreign body is difficult along with the bronchoscope. The circuit has to be disconnected to introduce the bronchoscope [1, 6]. We have used two nasal airways, one in each nostril and further connected it to the anaesthesia circuit via universal connector. There is no need to disconnect the circuit at any point[1]. The oral cavity was free to insert the bronchoscope and remove the foreign body orally. A correctly placed nasopharyngeal airway sits above the epiglottis and separates the soft palate from the posterior wall of the oropharynx. Thus it acts like a ‘splint’ which maintains patency of the airway by keeping the tongue from falling back on the posterior pharyngeal wall and occluding the airway, therefore preventing airway obstruction, hypoxia and asphyxia. In a study done by Aktham Adel Shoukry et al in 2018, they have compared the use of nasopharyngeal airway Versus Laryngeal Mask Airway during Diagnostic Flexible Fibre-Optic Bronchoscope in Children. They found that the use of NPA as supraglottic ventilating device for children undergoing diagnostic flexible fibreoptic bronchoscopy is considered a good alternative for shortening the bronchoscopy time with less incidence of hypoxemia and better recovery time compared to LMA[6]. In a study done by Qiansong Xiao et al in 2015, they have Comparison of Nasopharyngeal Airway Device and Nasal Oxygen Tube in Obese Patients Undergoing Gastroscopy under Intravenous Anaesthesia. SpO2 reduction during and after gastroscopy was significantly less in the group treated with the nasopharyngeal airway. This indicates that the nasopharyngeal airways are more able than the nasal oxygen tube to reduce airway obstruction and facilitate patient’s breathing. In addition, patients for whom the nasopharyngeal airway was used required significantly less emergent management. Simple management such as raising the mandible and supplying hyperbaric oxygen could reduce hypoxia [10]. However, violent insertion of the nasopharyngeal airway can result in injury to the upper nasal cavity. In the study done by Qiansong Xiao et al they found that adverse events such as movement, regurgitation and cough occurred in only 5.51% of the patients. The occurrence of adverse events in patientsin the nasopharyngeal airway group was comparable to that of patients in the nasal oxygen tube group. This suggests that use of the nasopharyngeal airway was well tolerated by patients, especially if its soft surface is lubricated with lidocaine gel [10, 11].
Conclusion
Use of nasal airway ventilation is a novel technique which can be used for maintaining the airway for bronchoscopic procedures, endobronchial ultrasound and interventional pulmonary procedures where procedure time is relatively prolonged.
References
1. Nasopharyngeal Airway versus Laryngeal Mask Airway During Diagnostic Flexible Fiber-Optic Bronchoscope in Children. Aktham Adel Shoukry*, Amr Gaber Sayed Sharaf. Bentham open.
2. Niggemann B, Haack M, Machotta A. How to enter the pediatric airway for bronchoscopy. Pediatr Int 2004; 46(2): 117-21.
3. Y. Bajaj, C. Gadepalli, and L. C. Knight, “Securing a nasopharyngeal airway,” Journal of Laryngology and Otology, vol. 122, no. 7, pp. 733–734, 2008.
4. A. R. Kumar, C. Guilleminault, V. Certal, D. Li, R. Capasso, and M. Camacho, “Nasopharyngeal airway stenting devices for obstructive sleep apnoea: a systematic review and meta-analysis,” Journal of Laryngology and Otology, vol. 129, pp. 2–10, 2015.
5. Du Rand IA, Blaikley J, Booton R, Chaudhuri N, Gupta V, Khalid S, Mandal S, Martin J, Mills J, Navani N, Rahman NM, Wrightson JM, Munavvar M; British Thoracic Society Bronchoscopy Guideline Group: Summary of the British Thoracic Society guideline for diagnostic flexible bronchoscopy in adults. Thorax 2013; 68:786-787.
6. The Safety of Laryngeal Mask Airway-Assisted Bronchoscopy versus Standard Nasal Bronchoscopy. Alon D.a, c · Pertzov B.b, c · Gershman E.b, c · Frishman M.a, c · Rahman N.A.b, c · Rosengarten D.b, c· Kramer M.R.b, c
7. Yserbyt J, De Maeyer N, Dooms C, Testelmans D, Muylle I, Bruyneel M, Ninane V: The feasibility of tracheal oxygen supplementation during flexible bronchoscopy. Respiration 2016; 92:48-52.
8. Gonzalez R, De-La-Rosa-Ramirez I, Maldonado-Hernandez A, et al. Should patients undergoing a bronchoscopy be sedated? Acta Anaesthesiologica Scand 2003; 47: 411–415.
9. Esther Vila, Anna Mases, Enrique Vela, Luis Molto, Albert Sanchez-Font, Víctor Curull and Lluís Gallart, Sedation with Propofol and remifentanil for real-time endobronchial ultrasound needle aspiration, Colombian Journal of Anesthesiology, 41, 2, (120), (2013).
10. Qiansong Xiao, Yingying Yang, Yinbin Zhou, Yan Guo, Xing Ao, Ran Han, Jiali Hu, Dongfeng Chen, and Chunhui Lan . Comparison of Nasopharyngeal Airway Device and Nasal Oxygen Tube in Obese Patients Undergoing Intravenous Anesthesia for Gastroscopy: A Prospective and Randomized Study. Gastroenterology Research and Practice Volume 2016, Article ID 2641257, 6 pages
11. T. Cavusoglu, I. Yazici, Y. Demirtas, B. Gunaydin, and R. Yavuzer, “A rare complication of nasotracheal intubation: accidental middle turbinectomy,” Journal of Craniofacial Surgery, vol. 20, no. 2, pp. 566–568, 2009.
12. Chadha M, Kulshrestha M, Biyani A. Anaesthesia for bronchoscopy. Indian J Anaesthesia 2015;59:565-73
13. Yarmus LB, Akulian JA, Gilbert C, et al. Comparison of moderate versus deep sedation for endobronchial ultrasound transbronchial needle aspiration. Ann Am Thorac Soc 2013; 10(2): 121-6.[http://dx.doi.org/10.1513/AnnalsATS.201209-074OC] [PMID: 23607840]
14. K Roberts1, H Whalley2, A Bleetman3. The nasopharyngeal airway: dispelling myths and establishing the facts. Emergency Medicine Journal. Volume 22, Issue 6.
15. Lida Fadaizadeh, Mahsa Sadat Hoseini, Mohammad Bagheri. Anaesthesia Management during Interventional Bronchoscopic Procedures: Laryngeal Mask Airway or Rigid Bronchoscope. Turk J Anaesth Reanim 2014; 42: 302-7
16. Grendelmeier P, Tamm M, Pflimlin E, Stolz D. Propofol sedation for flexible bronchoscopy: A randomised, noninferiority trial. Eur Respir J 2014; 43(2): 591-601.
17. Schade K, Borzotta A, Michaels A. Intracranial malposition of nasopharyngeal airway. J Trauma2000;49 (5) :967–8.
18. Chung CH, Sum CW, Li HL, et al. Comparison of nasal trauma associated with nasopharyngeal airway applied by nurses and experienced anesthesiologists. Changgeng Yi Xue Za Zhi1999;22 (4) :593–7.
| How to Cite this Article: Kanaparthi A, Nair V, Kale P, Kate A | Nasopharyngeal Airway As A Supraglottic Ventilation Device For Bronchoscopic Interventions | Journal of Anaesthesia and Critical Care Case Reports | Sep – Dec 2019; 5(3): 10-12. |
(Full Text HTML) (Download PDF)
.